Bell’s palsy in a case of Darier’s disease – a rare disease association or coincidental finding?
Kritika Pandey, Mankesh Lal Gambhir, Suresh Kumar Malhotra
Department of Dermatology, Venereology & Leprosy, Government Medical College, Amritsar, Punjab, India
ABSTRACT
Darier’s disease (DD) is a rare acantholytic dyskeratotic autosomal dominant genodermatosis characterized by the presence of warty, brown papules and plaques affecting the seborrhoeic areas. Frequent bacterial, fungal and viral particularly herpes simplex virus (HSV) infections complicate DD. Bell’s palsy is an acute onset, idiopathic facial paralysis resulting from a dysfunction anywhere along the peripheral part of the facial nerve. Reactivation of HSV is considered to be the main cause of Bell’s palsy. This case represents, to the best of our knowledge, the first case of DD presenting with Bell’s palsy. This case underlines the importance of recognizing HSV infection in DD.
Key words: Darier disease; Bell’s palsy; Skin disease
INTRODUCTION
Darier’s disease (DD) is an autosomal dominant condition characterized by a persistent eruption of hyperkeratotic papules, histological examination of which shows suprabasal acantholysis with dyskeratosis. Patients with DD have an increased susceptibility to herpes simplex infection. A number of clinical studies have described co-occurrence of various neurological and psychiatric symptoms with DD, but occurrence of Bell’s palsy with DD has never been reported [1]. We report here a case of DD with Bell’s palsy.
CASE REPORT
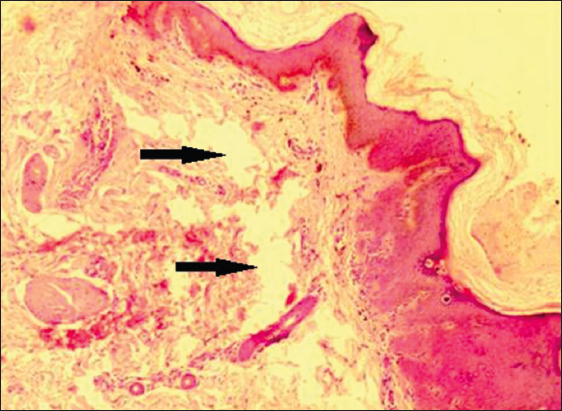
A 20 year old man presented with a 3-year history of itchy greasy yellow brown papules and plaques over face, neck, shoulders, upper back, axillae and groins (Fig. 1). On examination patient also had minute Palmar pits (Fig. 1) and V- shaped nicking of the free edge of the nails, characteristic of DD (Fig. 2). A skin biopsy was done from back to support clinical diagnosis, came consistent with diagnosis of DD (Fig. 3). Five days later, the patient presented with pain and weakness over right side of the face, was diagnosed as Bell’s palsy (Fig. 4) and treated with oral steroids and valacyclovir. Serological test for both HSV-1 and HSV-2 were non-reactive. A week later, there was improvement in both facial palsy and skin lesions (Fig. 5).




Prior to the study, patient gave written consent to the examination and biopsy after having been informed about the procedure.
DISCUSSION
Darier’s disease was described independently by White and Darier in 1889. It is an autosomal disorder with variable penetrance, related to mutations in ATP2A2 gene at chromosome 12q24.1, which encodes the sarco-endoplasmic reticulum calcium AT4Pase type 2 (SERCA2). This defect results in impaired intercellular adhesions [2,3].
It has world-wide distribution, with the prevalence estimated to vary from one in 36,000 to one in 100,000 and an incidence of new cases of four per million per 10 years [2,4].
Clinically, the distinctive lesions are firm, rather greasy, crusted papule that is skin-coloured or yellow–brown. Papules coalesce to produce irregular warty plaques or papillomatous masses, which, in the flexures, become hypertrophic, fissured and malodorous. Lesions are distributed in seborrhoeic pattern. The palms and soles may show punctate keratoses and minute pits. Nail changes include nail fragility, longitudinal ridging and splitting [2].
DD, either active or in remission, predisposes to some infectious complications, such as herpes simplex virus (HSV), varicella-zoster virus (VZV) and pox virus infections. It may present as atypical clinical presentation that frequently delay the recognition of viral infection and postpone adequate antiviral treatment. Increase in the susceptibility to various infections in Darier’s disease has been linked to impaired cellular and/or humoral immunity [5].
Bell’s palsy the most common disease of facial nerve, is an acute idiopathic peripheral facial paralysis. It is the cause of 60-75% of cases of unilateral facial paralysis with incidence of 20-30 cases per 100,000 per year [6].
The diagnosis can be easily established in patients with unexplained unilateral isolated facial weakness. The onset is sudden and symptoms typically peak within a few days. Additional symptoms may include pain in or behind the ear, numbness or tingling in the affected side of the face usually without any neural deficit, hyperacusis and disturbed taste on the ipsilateral anterior part of the tongue [7].
Autoimmune process, viral infections, and even ischemia are the cause of initiation of inflammation. Different viruses from herpes virus family, herpes simplex virus -1 (HSV-1), HSV-2, human herpes virus -6 (HHV-6), and varicella zoster virus (VZV) have been considered to play role in bell’s palsy. HSV has been considered particularly as the etiological agent in recent studies. Despite studies in favour of seropositivity of HSV in Bell’s palsy, most studies could not find any definite association between antibody titres and Bell’s palsy [8,9].
The main aim of treatment in the acute phase of Bell’s palsy is to speed up the recovery and to prevent corneal complications. Strategies to speed recovery include physical therapy, corticosteroids and antiviral agents. Inflammation and edema of the facial nerve are implicated in causing Bell’s palsy. The rationale for the use of corticosteroids in acute phase of Bell’s palsy is that they have a potent anti-inflammatory action which should minimize nerve damage and thereby improve the outcome. The rationale for the use of antiviral agents is the evidence that the inflammation of the facial nerve in Bell’s palsy might be related to the HSV [10].
CONCLUSION
This case represents, to the best of our knowledge, the first case of DD presenting with Bell’s palsy. The cause of Bell’s palsy in this case, whether it is the reactivation of HSV due to disease per se or due to stress after skin biopsy remains eluded. This case underlines the importance of recognizing HSV infection in DD and also highlights the possible therapeutic effect of anti-viral agents in DD.
Consent
The examination of the patient was conducted according to the Declaration of Helsinki principles.
REFERENCES
1. Jacobsen NJO, Lyons I, Hoogendoorn B, Burge S, Kwok PY, O’Donovan MC, ATP2A2 Mutations in Darier’s Disease and Their Relationship to Neuropsychiatric PhenotypesHum Mol Genet 1999; 8: 1631-6.
2. Burge SM, Wilkinson JD, Darier-White disease: a review of the clinical features in 163 patientsJ Am Acad Dermatol 1992; 27: 40-50.
3. Sakuntabhai A, Ruiz-Perez V, Carter S, Jacobsen N, Burge S, Monk S, Mutations in ATP2A2, encoding a Ca2+pump, cause Darier diseaseNat Genet 1999; 21: 271-7.
4. Tavadia S, Mortimer E, Munro CS, Genetic epidemiology of Darier’s disease: a population study in the west of ScotlandBr J Dermatol 2002; 146: 107-9.
5. Nikkels AF, Beauthier F, Quatresooz P, Piérard GE, Fatal herpes simplex virus infection in Darier disease under corticotherapyEur J Dermatol 2005; 15: 293-7.
6. Gilden DH, Bell’s PalsyNew England J Med 2004; 351: 1323-31.
7. Hauser WA, Karnes WE, Annis J, Kurland LT, Incidence and prognosis of Bell’s palsy in the population of Rochester, MinnesotaMayo Clin Proc 1971; 46: 258-64.
8. Harirchian1 MH, Sarrafnejad A, Ghaffarpour M, Ghelichnia H, Herpes simplex virus in saliva of patients with Bell’s palsyActa Medica Iranica 2008; 46: 5-10.
9. Furuta Y, Fukuda S, Chida E, Takasu T, Ohtani F, Inuyama Y, J Med Virol1998; 54: 162-6.
10. Murthy JM, Saxena AB, Bell’s palsy: Treatment guidelinesAnn Indian Acad Neurol 2011; 14: Suppl 1S70-2.
Notes
Source of Support: Nil,
Conflict of Interest: None declared.
Comments are closed.