An unusual misleading multiple nodules on the extremities – a case report
Kiruba Dheenadhayalan, Sundaramoorthy Srinivasan, Sowdhamani Bakthavatsalam
Chettinad Hospital and Research Institute, Kelambakkam, Tamilnadu, India
ABSTRACT
Benign fibrous histiocytoma is a common benign dermal neoplasm mainly composed of a mixture of fibroblastic and histiocytic cells. It is also known as dermatofibroma, sclerosing haemangioma, or nodular subepidermal fibrosis. There are many histological variants of fibrous histiocytoma such as aneurysmal, cellular, epitheloid, atypical, keloidal and palisading subtypes. The diagnosis of cutaneous benign fibrous histiocytoma is generally easy; however, rare variants may be difficult to identify and the diagnosis can only be confirmed after histopathological examination and by immunohistochemical staining. We report a case of 52 yr old woman with asymptomatic multiple pigmented raised skin lesions over both lower limb and right arm which was histopathologically diagnosed as atypical benign fibrous histiocytoma(ABFH) involving subcutaneous tissue and the immunohistochemical staining was done and the treatment was proceeded with complete wide surgical excision due to its higher tendency to recur locally and the patient was advised for regular follow up.
Key words: Dermatofibroma, Atypical fibrous histiocytoma, fibrous histiocytoma.
INTRODUCTION
Dermatofibroma (DF), originally described by Unna [1] in 1894 [2], is a common benign dermal neoplasm formed by proliferation of histiocytes and fibroblast, so also called as benign fibrous histiocytoma) [3]. They usually present with solitary or multiple, flesh coloured to brown, firm, asymptomatic or mildly tender papule, plaque or nodule of 1cm in diameter with tethering of the overlying epidermis to the underlying lesion. On lateral compression of lesion they show a dimpling over the surface known as “dimple sign” or “button holing”. Most common on extremities, especially the lower limbs and often seen in women [4]. There are numerous clinicopathological variants such as cellular, aneurysmal, atypical, epitheloid, atrophic, lichenoid, keloidal and ulcerative fibrous histiocytoma [5–7] out of which our case presented with a rare group of atypical benign fibrous histiocytoma.
CASE REPORT
A 52 year old lady came with c/o asymptomatic multiple pigmented raised skin lesions over her right arm and both lower limbs since 5 years. Initially started as a single lesion over her left leg which then gradually increased in number and started to involve the other leg & Rt arm over the past 1 year. H/o topical application of clobetasol with salicylic acid cream over the lesion for 3 weeks present but did not showed any change in lesion except the surrounding skin hypo pigmentation. The patient had no h/o trauma prior or any other significant medical problem.
On examination, multiple well defined oval hyperpigmented nodules of varying size of 2 cm× 1.5 cm present over anterior aspect of right arm and medial as well as lateral aspect of both lower limbs. On palpation, it was firm, non tender, mobile with tethering of skin to underlying structure and dimpling was present on lateral pressure of the lesion (Figs. 1 and 2).


Routine investigations like CBC, LFT, RFT, Urinalysis, serology was within normal limit. We arrived into a differential diagnosis of dermatofibroma, malignant melanoma, atypical dysplastic nevus, angioma and fibrous xanthogranuloma.
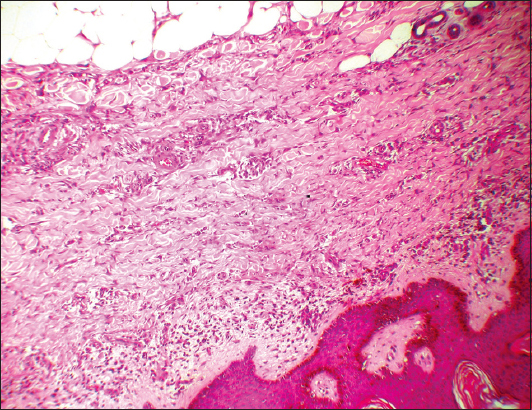
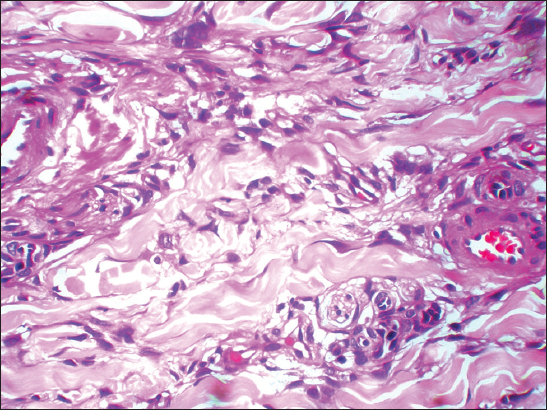
Although the initial clinical diagnosis was dermatofibroma, establishing a conclusive diagnosis was difficult initially. A wide local excisional biopsy of single lesion was done which revealed atypical benign fibrous histiocytoma with feature of mild irregular acanthosis &dermis showed ill defined lesion comprised of spindle cells which exhibit mild atypia and giant cells. These cells were surrounded by collagen bundles and the lesions were extending upto subcutaneous tissue (Figs. 3 and 4) and later immunohistochemical staining was done which showed CD 34 negative and positive for Factor XIIIa and vimentin.
Prior to the study, patient gave written consent to the examination and biopsy after having been informed about the procedure.
DISCUSSION
Atypical benign fibrous histiocytoma (ABFH) was first described by Fukamizu et al in 1983. It is also known as atypical fibrous histiocytoma or dermatofibroma with monster cell [8]. It is due to proliferation of fibroblastic and histiocytic cells, occurs frequently in the dermis. A deep penetrating type involving subcutaneous tissue is usually rare comprising less than 2% of all FH [9]. They usually occurs as a nodule on the lower extremities, especially in adults with male predominance [7,10].
Histopathological variants like cellular, atypical, aneurysmal DF as well as dermatofibroma arising on the face, subcutaneous and deep soft tissues have an increased risk for local recurrence (upto 20%) and have been reported to metastasize to the lymph node and lungs and even caused death in some patients [11–13]. Out of all these AFH alone tends to show a higher recurrence rate of 14% than ordinary fibrous histiocytoma (2-3%) and even rare metastases have been described [7,11,14,15].
Interestingly, our case reported herein was clinically characterized by the presence of multiple lesions, involving both upper as well as lower extremities, histopathologically revealed an unusual atypical variant of DF with invasion of atypical cells into the subcutaneous tissue. Immunohistochemical staining showed positivity for factor XIIIa and vimentin and negativity for CD34 thus differentiates ABFH from dermatofibrosarcoma protuberans [9,15].
As per the treatment modality, all the tumors was surgically excised completely with clear margins and the patient was adviced for regular follow up.
CONCLUSION
ABFH is a poorly recognized variant of fibrous histiocytoma which usually lacks a clear cut predictive morphological pattern. Recognition of this variant is important because it has high potential for local recurrence and metastasis and so, a complete surgical excision and regular follow up is recommended in all cases after the final diagnosis.
REFERENCES
1. Unna PG, Histopathologie der Hautkrankheiten 1894; Berlin: August Hirschwald; 839-42.
2. Thappa MD, Multiple dermatofibromas with unusual featuresIJDVL 1995; 61: 120-2.
3. Levine N, Levine CC, A-Z essentials dermatology therapySpringer-Verlag Berlin Heidelberg 2004; 180.
4. Fitzpatrick dermatology in general medicine 2008; Vol 1: seventh edition. section 9556-7.
5. Fletcher CD, Benign fibrous histiocytoma of subcutaneous and deep soft tissues: A clinicopathologic analysis of 21 casesAm J Surg Pathol 1990; 14: 801-9.
6. Ferrari A, Argenziano G, Typical and atypical dermoscopic presentations of dermatofibromaJEADV 2013; 27: 1375-80.
7. Rook A, Textbook of dermatology 2010; vol 3: eighth edition. chapter 5656.16.
8. Ishitsuka Y, Ohara K, Atypical fibrous histiocytoma of the skin with necrobiotic granuloma like featuresActa Derm Venerol 2011; 91: 482-3.
9. Garrido Ruiz MC, Subcutaneous atypical fibrous histiocytomaAm J Dermatopathol 2009; 31: 499-501.
10. Kamino H, Jacobson H, Dermatofibroma extending into the subcutaneous tissueAm J Surg Pathol 1990; 14: 1156-64.
11. Kaddu S, McMenamin ME, Fletcher CDM, Atypical fibrous histiocytoma of the skin. Clinicopathologic analysis of 59 cases with evidence of infrequent metastasisAm J Surg Pathol 2002; 26: 35-46.
12. Gleason BC, Fletcher CDM, Deep ‘benign’ fibrous histiocytoma: clinicopathologic analysis of 69 cases of a rare tumor indicating occasional metastatic potentialAm J Surg Pathol 2008; 32: 354-62.
13. Mentzel T, Wiesner T, Cerroni L, Hantschke M, Kutzner H, Rütten A, Malignant dermatofibroma: clinicopathological, immunohistochemical, and molecular analysis of seven casesMod Pathol 2013; 26: 256-67.
14. Leyva WH, Santa Cruz DJ, Atypical cuataneous fibrous histiocytomaAm J Dermatopathol 1986; 8: 467-71.
15. IADVL. Textbook of dermatology 2008; vol 2: third edition. 1509-1510.
Notes
Source of Support: Nil,
Conflict of Interest: None declared.
Comments are closed.