Sebaceoma of the lip originating in Fordyce’s spot – A rarity
Anuradha Calicut Kini Rao1, Bhavna Nayal1, Sushmitha Malpe Gopal2, Manna Valliathan1, Rajgopal Shenoy3
1Department of Pathology, Kasturba Medical College, Manipal, Manipal University, Karnataka, India, 2Department of Pathology, Melaka Manipal Medical College, Manipal, Manipal University, Karnataka, India[3]Department of Surgery, Kasturba Medical College, Manipal, Manipal University, Karnataka, India
ABSTRACT
Introduction: Sebaceomas are relatively rare benign neoplasms differentiating towards sebaceous glands. These dermal neoplasms present as solitary papule or nodule. The age of presentation is sixth to ninth decade with a female preponderance. They may be associated with underlying visceral malignancies. We present a case of sebaceoma of the lip. This case is being presented because of its rare site of occurrence.
Case report: A seventy five year old lady presented with a single, well defined, painless and progressively enlarging flesh coloured papule over the upper lip of two months duration. No systemic signs or symptoms suggestive of visceral malignancy were present. Clinical diagnosis of papilloma was proferred. Histopathological examination of the excision biopsy revealed nests and lobules of basaloid cells and few mature sebocytes seeming arising from central hyperplastic sebaceous gland. Final diagnosis of sebaceoma was rendered.
Conclusion: Sebaceoma is an adnexal tumour typically affecting the face and the scalp. To the best of our knowledge, this is the first case to be reported in literature in the lip. The possible origin of sebaceoma in the present case could be ectopic sebaceous glands (Fordyce’s spots) which occur in increasing frequency in elderly individuals, especially in the lip.
Key words: Sebaceoma, lip, papule, Fordyce’s spot, papilloma
INTRODUCTION
Sebaceomas are uncommon benign dermal lesions [1]. Troy and Ackerman coined the term sebaceoma to describe what was earlier known as sebaceous epithelioma, two decades ago [1,2]. Sebaceoma is a benign sebaceous tumour with >50% basaloid cell content. Sebaceoma is usually not suspected clinically due to its rarity [1]. Clinically, it presents as solitary papule or nodule on the face and scalp affecting elderly individuals with a female preponderance [2]. Sebaceoma may be associated with visceral malignancies. Sebaceoma is characterised by variably sized lobules composed of basaloid cells along with single or clustered mature sebaceous cells, and exhibit sebaceous ductal differentiation [3]. Fordyce’s spots are ectopically located sebaceous glands, more common on the vermillion border of the upper lip [4].
We present a case of sebaceoma arising in Fordyce’s spot which is a rarity.
CASE REPORT
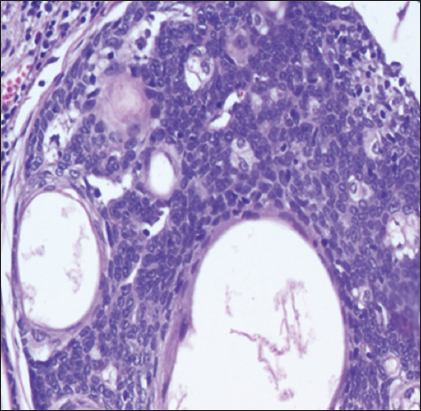
A 75 five year old lady presented to the surgical clinic with a single asymptomatic papule over the upper lip since two months. On clinical examination, the papule was well defined, flesh coloured and painless. There was no evidence of visceral or any other malignancy. Clinical diagnosis of papilloma was given. The lesion was excised. The specimen received in the pathology department measured 0.5×0.5×0.5cm weighed <1 gms and was dome shaped single skin covered tissue bit, cut section of which showed grey white areas. Microscopically, a well circumscribed, symmetrical dermal lesion was noted, around a central sebaceous gland which showed hyperplasia of the basaloid cells and was continuous with the tumor (Fig. 1). The tumour was composed of closely packed nests and lobules of basaloid cells with few vacuolated mature sebocytes along with duct like structures (Fig. 2). Based on all these features the final histopathological diagnosis of sebaceoma was given.

Prior to the study, patient gave written consent to the examination and biopsy after having been informed about the procedure.
DISCUSSION
Sebaceomas are benign sebaceous neoplasms presenting as a solitary yellow to flesh-colored papule on the face and scalp of elderly females [2]. Histopathological examination is characterized by a dermal tumor consisting of multiple variably sized discrete lobules composed predominantly of basaloid cells, admixed with single or clustered mature sebaceous cells lacking an organized lobular architecture separated by dense eosinophilic connective tissue. The basaloid cells are typically small and uniform with round to oval nuclei. Absence of nuclear pleomorphism, stromal retraction, peripheral palisading and sparse mitotic activity is typical. The sebaceous cells are mature, with eosinophilic bubbly cytoplasm and scalloped nuclei. Sebaceous ductal differentiation and cyst formation are common features [2,3]. Stromal retraction and peripheral palisading are absent. Epidermal involvement is sometimes seen [2]. Foci of squamous metaplasia may rarely be seen [3].
A verrucous variant of sebaceoma has been separated from the classical sebaceoma based on the connection with a hyperplastic infundibulum in the upper portion of the lesion, prominent granular layer and basosquamous differentiation. Its architecture and cytology are however similar [3,5].
Classical sebaceoma has to be differentiated from sebaceous adenoma, sebaceous carcinoma, and basal cell carcinoma with sebaceous differentiation and trichoblastoma with sebaceous differentiation on histopathological examination [2].
Sebaceous adenomas and sebaceomas can be considered as two ends of a spectrum of benign sebaceous neoplasia, with the former being more organoid while the latter shows extensive basaloid differentiation. [1]. Histopathologically, sebaceous adenoma is a well-circumscribed dermal nodule formed of lobules of predominate central mature, bland sebaceous cells with peripherally located one or two layers of germinal basaloid epithelial cell. There is no central draining duct [3]. The central sebocytes are larger with eosinophilic bubbly cytoplasm, although indentation of the nuclei is often less prominent. There can be connection with the overlying squamous epithelium [1].
Sebaceous carcinomas show irregular lobular patterns with evidence of asymmetry, poor circumscription, and infiltrative growth pattern with preponderance of pleomorphic, basaloid cells that are arranged in solid sheets showing cytonuclear atypia, high mitotic activity and necrosis which is not seen in sebaceoma [2,3]. Scattered sebocytes are often present within the basaloid tumour mass. Peripheral palisading and artefactual clefting are absent [3].
Some authors believe that sebaceoma is synonymous with basal cell carcinoma (BCC) with sebaceous differentiation. BCC with sebaceous differentiation is similar to classical BCC, but with a component of sebaceous differentiation [3]. Sebaceomas can be differentiated from basal cell carcinoma with sebaceous differentiation as the latter shows aggregate of follicular germinative basaloid cells composed of pleomorphic basaloid cells showing brisk mitotic activity along with distinct peripheral basal cell palisading, loose fibromucinous stroma, focal sebaceous differentiation, basaloid tumour necrosis and tumour–stroma separation artefact in formalin fixed sections [3,4].
Histopathologic features of trichoblastoma with sebaceous differentiation are those of the large nodular type of trichoblastoma characterized by large nodular aggregations composed of follicular germinative cells with palisading borders and highly fibrotic stroma, Limited differentiation toward follicular germs and rudimentary papillae is seen. In addition to these features, sebocytes and sebaceous duct-like structures are observed within the basaloid aggregations [5].
Sebaceoma can occur in association with Muir–Torre syndrome, an autosomal dominantly inherited disorder characterised by visceral malignancies (colorectal, upper gastrointestinal, endometrial and urological malignant neoplasms), tumours of sebaceous glands or keratoacanthoma [3]. But in this case no associated visceral malignancies or any other tumours were observed.
Lazar et al mentions that the common sites of sebaceoma are the head and neck area [1]. In a study by Misago et al, the most common site of sebaceoma is the head [5]. In the present case, the site of sebaceoma is the Fordyce’s spot in the upper lip.
Fordyce’s spots are ectopically located sebaceous glands described by Fordyce in 1896. The common sites of Fordyce’s spots are lips, oral mucosa and rarely genital mucosa. JH Lee, et al reported a male predilection for Fordyce’s spots, with most patients in their early or middle adulthood. Previous studies have reported female predilection for Fordyce’s spots involving the elderly patients. In the present case, Fordyce’s spot is involving an elderly female patient [4].
Studies have documented that the most common site of involvement of Fordyce’s spots is vermilion border of the upper lip with most patients presenting with asymptomatic tiny papules and plaques. In the present case, the patient presented with asymptomatic papule over the upper lip. On histopathology examination, Fordyce’s spots shows normal sebaceous gland composed of single sebaceous lobule or gland which consists of small clusters of mature sebocytes with a sebaceous duct, opening directly onto the epithelial surface which is located in the dermis or submucosa [4]. In the present case, Fordyce’s spot showed features of sebaceoma which is a rarity.
CONCLUSION
- To the best of our knowledge, this is the first case of sebaceoma to be reported in literature in the lip
- The possible origin of sebaceoma in the present case could be ectopic sebaceous glands (Fordyce’s spots)
Consent
The examination of the patient was conducted according to the Declaration of Helsinki principles.
REFERENCES
1. Lazar AJ, Lyle S, Calonje E, Sebaceous neoplasia and Torre -Muir syndromeCurr Diagn Pathol 2007; 13: 301-19.
2. Too EY, Wang YS, Fleshy Facial Lesion on an 80-Year-Old Dayak WomanArch Dermatol 2009; 145: 1325-30.
3. Alsaad KO, Obaidat NA, Ghazarian D, Skin adnexal neoplasms—part 1: An approach to tumours of the pilosebaceous unitJ Clin Pathol 2007; 60: 129-44.
4. Lee JH, Lee JH, Kwon NH, Yu DS, Kim GM, Park CJ, Clinicopathologic Manifestations of Patients with Fordyce’s SpotsAnn Dermatol 2012; 24: 103-6.
5. Misago N, Mihara I, Ansai S, Narisawa Y, Sebaceoma and related neoplasms with sebaceous differentiation: a clinicopathologic study of 30 casesAm J Dermatopathol 2002; 24: 294-304.
Notes
Source of Support: Nil,
Conflict of Interest: None declared.
Comments are closed.