Dermatology Eponyms – sign –Lexicon (Q)
Piotr Brzeziński13, Jana Zímová2, Ewelina Cywinska3, Anca Chiriac45
1Department of Dermatology, 6th Military Support Unit, Ustka, Poland, 2Department of Dermatology, University Hospital Ostrava, 17. listopadu 1790, 708 52 Ostrava-Poruba, Czech Republic, 3“Trychoderm” Clinic, ul. Kossaka 22, Slupsk, Poland, 4Department of Dermatology, Nicolina Medical Center, Iasi, Romania, 5Department of Dermato-Physiology, Apollonia University Iasi, Strada Muzicii nr 2, Iasi-700399, Romania
ABSTRACT
Eponyms are used almost daily in the clinical practice of dermatology. And yet, information about the person behind the eponyms is difficult to find. Indeed, who is? What is this person’s nationality? Is this person alive or dead? How can one find the paper in which this person first described the disease? Eponyms are used to describe not only disease, but also clinical signs, surgical procedures, staining techniques, pharmacological formulations, and even pieces of equipment. In this article we present the symptoms starting with (Q) and other. The symptoms and their synonyms, and those who have described this symptom or phenomenon.
Key words: Eponyms, Skin diseases, Sign, Phenomenon
Q SIGN
Endocarditis, pneumonia, fever, and liver involvement caused by the zoonotic Coxiella burnetii found in many mammals, including cattle, sheep, cats, dogs, rodents, birds, and ticks. Also called Q or Query Fever [1].
QUARTER EVIL SIGN
Symptomatic Anthrax [2]
This is found in certain cases of disease in cattle, having a rapid course and nearly always a fatal issue. The disease has several names, such as “Black-leg,” “Quarter evil,” and, in Germany, “Rauschbrand”.
The bacilli are thickish rods, which are mostly single. They have lively motion by means of numerous cilia. The bacillus grows readily on ordinary media, but it is strictly anaerobic. It produces spores which are thicker than the bacillus and lie nearer one end than the other, so that a somewhat club-shaped form is produced. It produces gas in stab-cultures, and is decolorized when treated by Gram’s method, in both these respects contrasting with bacillus anthracis.
QUECKENSTEDT SIGN
An indication of the existence of something; any objective evidence of a disease, ie, such evidence as is perceptible to the examiningphysician, as opposed to the subjective sensations (symptoms) of the patient [3,4].
QUEEN ANNE SIGN
In hypothyroidism, sparse eyebrows laterally (loss of outer eyebrows 2/3).
Apparently it was fashionable to shave the lateral third of the eyebrow during the region of Queen Anne (1701-1714) in Great Britain [5]. The association with Anne of Denmark is based on portraiture, although history does not suggest that she suffered an underactive thyroid. The eponym is disputed by some, though it has been suggested that Anne of France, Anne of Brittany, Anne of Austria, Anne Boleyn and Anne of Cleves may all be eliminated as candidates [5,6]. Known as sign of Hertoghe [7,8].
QUEEN ANNE
Anne of Denmark (1574-1619) was Queen consort of Scotland, England, and Ireland as the wife of James VI and I.
Anne of Cleves (German: 1515 -1557) was Queen of England from 6 January 1540 to 9 July 1540 as the fourth wife of King Henry VIII.
Anne Boleyn (c. 1501-1536) was Queen of England from 1533 to 1536 as the second wife of King Henry VIII and Marquess of Pembroke in her own right.
Anne of Austria (1601-1666) was queen consort of France and Navarre, regent for her son, Louis XIV of France, and a Spanish and Portuguese Infanta by birth.
Anne of Brittany (1477-1514) was a French queen who reigned as Duchess of Brittany from 1488 until her death.
Anne of France (or Anne de Beaujeu) (1461-1522) was the eldest daughter of Louis XI of France and his second wife, Charlotte of Savoy [9,10].
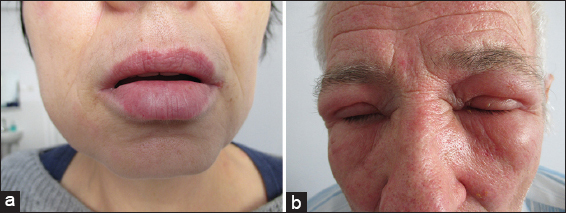
QUINCKE’S SKIN SIGN, GIANT URTICARIA; URTICARIA OEDEMATOSA
Quincke’s edema or Angioedema is the rapid swelling (edema) of the dermis, subcutaneous tissue, mucosa and submucosal tissues (Fig. 1a and b). It is very similar to urticaria, but urticaria, commonly known as hives, occurs in the upper dermis [11,12].
HEINRICH IRENAEUS QUINCKE
German physician, 1842-1922 (Fig. 2). He was educated in Berlin where he also completed his medical studies in 1864. After a ‘grand tour’ that took him to Paris, Vienna and London, he was trained in Berlin, first in surgery and later in internal medicine, under Von Frerichs (1819-1885). In 1878, he became a professor of internal medicine in Berne; from 1883 he held the chair of medicine in Kiel, which he would hold for the next 30 years.
In 1882, he published a synthesis of several observations of ‘acute, circumscribed oedema of the skin’. Quincke accurately described the clinical features and distinguished the familial from the sporadic forms. He was correct in attributing the condition to increased vascular permeability, but he surmised the causal factors were neurogenic rather than humoral, according to current insights (excess of bradykinin due to external factors or hereditary deficiency of C1-esterase inhibitor). Quincke not only contributed to several other clinical observations, but also pioneered the lumbar puncture, initially not for diagnostic purposes, but to relieve headache in hydrocephalic children [13,14].
QUINCKE’S SIGN
A blanching of the fingernails at each diastole of the heart. A sign seen in aortic insufficiency [11].
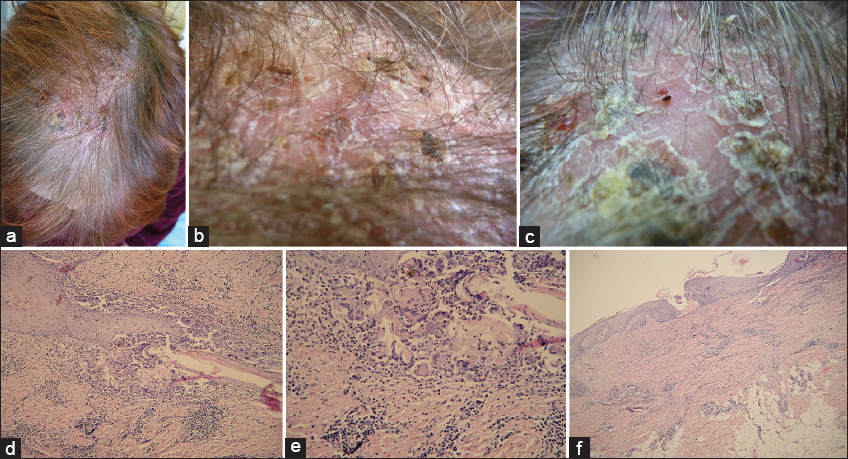
QUINQUAUD’S SCALP SIGN
A purulent folliculitis of the scalp, causing irregular bald patches (Figs 3a – f). Folliculitis decalvans is a rare inflammatory scalp disorder. [15–18]. Folliculitis decalvans was first described by Quinquaud in the 1888. He reported one case of “folliculite épilante et destructive des regions velues” in 1888 [17]. He investigated three similar cases of pustular scarring alopecia and isolated bacteria from the hair follicle. Quinquaud transferred the bacteria to rats, mice, and rabbits but was not able to provoke a similar response in their fur. Brocq et al. in 1905 described Quinquaud’s clinical findings under the designation “folliculitis decalvans” and distinguished it from other types of cicatricial alopecia [16].
CHARLES EUGENE QUINQUAUD
French physician (1841-1894) (Fig. 4). Charles Eugene Quinquaud entered medical school at Limoges in 1864 and in 1868 moved to Paris, where he obtained his doctorate in 1873. He was the last Interne des hôpitaux under Pierre Antoine Ernest Bazin (1807-1878) and it was Bazin who influenced him to study dermatology. He became médecin des hôpitaux in 1878, agrégé in 1883, and in 1886 chef de service at the Hôpital Saint-Louis, with Ernest Henri Besnier (1831-1909), Jean Alfred Fournier (1832-1915), and Jean Baptiste Emile Vidal (1825-1893) as colleagues. He was elected member of the Académie de Médecine in 1892.
Quinquaud contributed to many areas of medicine, being a skilled bacteriologist as well as a clinician, and with Nestor Gréhant (1838-1910) he developed a method for measuring blood volume using carbon monoxide (1882). He gave popular courses in internal medicine and pathology as well as dermatology and unselfishly supported Louis Brocq, enabling him to teach and see patients despite considerable opposition by some who were jealous of this young man’s meteoric success and popularity.
In 1880, 1885, and 1887 Quinquaud won academic prizes for his works. He was editor of the journal La médecine scientifique [19].
REFERENCES
1. Muniain Ezcurra MA, Gálvez-Acebal J, Q fever and fever of unknown origin. Are the chronic forms of these conditions preventable?Rev Clin Esp 2015; 215: 274-5.
2. Kunii O, Kita E, Shibuya K, [Epidemics and related cultural factors for Ebola hemorrhagic fever in Gabon]Nihon Koshu Eisei Zasshi 2001; 48: 853-9.
3. Deliyannakis E, Influence of the position of the head on the cerebrospinal fluid pressure. Variations of the Queckenstedt signMil Med 1971; 136: 370-2.
4. Ikebe S, Yokochi F, Wada T, Arakawa A, Mori H, Suda K, [A 66-year-old man with backache and progressive difficulty of gait]No To Shinkei 1993; 45: 981-90.
5. Keynes M, Letter to the editorJ Med Biogr 2009; 17: 62.
6. Lane Furdell E, Eponymous, anonymous: Queen Anne’s sign and the misnaming of a symptomJ Med Biogr 2007; 15: 97-101.
7. Brzezinski P, Pessoa L, Galvão V, Barja Lopez JM, Petrovitch Adaskevich U, Niamba PA, Dermatology Eponyms – sign –Lexicon (H)Our Dermatol Online 2013; 4: 130-43.
8. Al Aboud K, Medical Eponyms linked to hairOur Dermatol Online 2012; 3: 377-8.
9. Ross J, Queen Anne (1665-1714) and her healthJ Med Biogr 2015; 23: 54-9.
10. Regöly-Mérei G, [Paleopathological study of the remains of Béla the Third, King of Hungary, and his wife, Queen Anne]Orv Hetil 1968; 109: 423-7.
11. Giavina-Bianchi P, Aun MV, Motta AA, Kalil J, Castells M, Classification of angioedema by endotypesClin Exp Allergy 2015; 45: 1142-3.
12. van Gijn J, Gijselhart JP, [Quincke and his oedema]Ned Tijdschr Geneeskd 2012; 156: A5238.
13. Cozanitis DA, Heinrich Irenaeus Quincke (1842-1922): the Nobel Prize but for the problem of agePresse Med 2013; 42: 464-70.
14. Minagar A, Lowis GW, Dr Heinrich Irenaeus Quincke (1842-1922): clinical neurologist of KielJ Med Biogr 2001; 9: 12-5.
15. Faye I, Marchand JP, N’Diaye B, Sarrat H, [Atypical form of Quinquaud’s folliculitis decalvans]Bull Soc Med Afr Noire Lang Fr 1973; 18: 189-90.
16. Otberg N, Kang H, Alzolibani AA, Shapiro J, Folliculitis decalvansDermatol Ther 2008; 21: 238-44.
17. Quinquaud E, Folliculite epilante et destructive des regions veluesBull Mem Soc Hop Paris 1888; 5: 395-8.
18. Zímová J, Pock L, Folliculitis decalvans capillitiiDermatol Praxi 2012; 6: 26-8.
Notes
Source of Support: Nil
Conflict of Interest: None declared.
Comments are closed.