The use of a topical compound cream product with chitosan, silver sulfadiazine bentonite hidrogel and lactic acid for the treatment of a patient with rosacea and ulcerated livedoid vasculopathy
1Faculty of Medicine and Pharmacy, University, Dunarea de Jos, Galati, Romania, 2Private Practice, Galati, Romania
ABSTRACT
Introduction: The aims of this study were to investigate the use of a topical compound cream product with Chitosan, Silver Sulfadiazine, Bentonite hidrogel and Lactic acid for the treatment of a patient with Rosacea and prolonged ulcerated Livedo Vasculitis.
Methods: A patient with ulcerated Livedo Vasculitis applied the cream 22 months daily and was examined clinically.
Results: At five months the area of the right foot ulcer decreased to a diameter of 18 mm. The pain disappeared (anamnestically) in 7 days around the ulcerated areas reticulated atrophic hipopigmented areas were seen-atrophie blanche and there ware still 4 small ulcerations. I noted also the disappearance of the livedoid area from the middle of the second toe finger. The left foot ulcer was epithelised. Wound cultures were negative. After another five months of continues use of the topical cream the situation improves, diameter of the ulcer decreased at 13 mm, the small ulcerations disappeared but continues to stay on the right foot. After another year the situation is stable at the right foot but the left ulcer was partially recurrent and it was painful.
Conclusions: The topical compound formula with four active ingredients: Silver sulfadiazine, bentonite hidrogel, chitosan and lactic acid it was a cheap treatment for the patient, it was tolerated without sensitizing even it was used continuously for 22 months.
Key words: Livedoid vasculitis; Chronic ulcer; Topical compound cream; Silver sulfadiazine; Chitosan; Bentonite
INTRODUCTION
Livedoid vasculopathy is a disease of the lower legs with painful chronic ulcerations and cutaneous atrophy blanche located particularly around the malleoli and commonly seen on adult women. I present a case of a 39 years old man with Rosacea and dorsoplantar chronic and painful ulcerations known with the disease and referred to me for a topical treatment as he was partially refractory to systemic therapies and also to local ones. I used a compound topical cream product which contains chitosan, argentic sulfadiazine, bentonite and lactic acid with good result and tolerance. The ulceration decreased and the pain was disappeared.
CASE REPORT
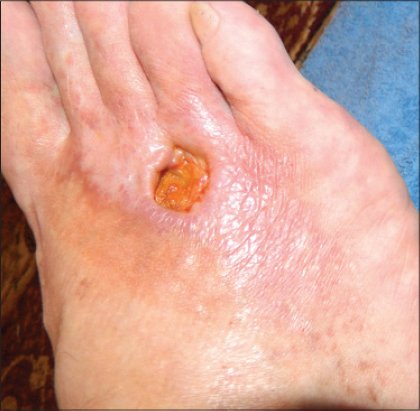
A 39 years old man was referred to my Private Practice from the Vascular Surgery unit with a long history -7 years-of painful ulcerations on the dorsoplantar areas and sometime around maleoli. The patient was previously consulted those years by dermatologists, vascularsurgeons, internists and the Diagnosis of livedoid vasculopathy was established before but now he said is the most painful period and he needed help for the wound to heal. The patients history reveals Rosacea and hypercholesterolemia. Previously he was treated in time with low –dose aspirin, dipyridamole, pentoxyphylline, fraxiparine. At the time of the referral he was on treatment with rosuvastatin 20mg daily and clopidogrel 75 mg daily, he used topically on ulcers silver dressings and for the face metronidasole cream. He had no history of smoking or of thrombosis and no varicous visible veins. Physical examination revealed one large (66mm of diameter) painful ulceration on dorsoplantar area of the right foot, with some edema and circular erythema around it and also a livedoid area on the second toe finger (Fig. 1). On the surface of the ulcer there was a detritus with the rest of previous treatments, pus and scales. The second ulceration was in perimaleolar area of the foot (8 mm of diameter) (Fig. 2). Wound cultures from both ulcers showed Klebsiella with maximum sensitivity to Cefixime. Venous ultrasound was normal. He had two previous biopsys consistent with stasis, fibrosis, hyalinization of the vessels, the PAS (Periodic Acid Schiff) taining was negative, thrombosis of the superficial vessels, red blood cell extravasation suggesting the diagnosis of livedoid vasculopathy. The tests for Protein C, Protein S, homocysteine, antithrombine III, Lupusanticoagulant, Cryoglobulines, Cholesterol, Anticardiolipine, antibodies, anti –double-stranded DNA antibodies, complement, prothrombin time/partial thromboplastin time, aspartate aminotransferase/alanine aminotransferase, were within normal limits or negative [1]. The Erythrocyte sedimentation rate was elevated at 42 mm/hr.


I added at his previous treatment Cefixime 400 mg daily for 10 days and after the informed consent was signed and the Institutional Review board approval was taken, we advise the patient to apply once a day a combination product containing chitosan, argenticsulfadiazine, bentonite and lactic acid (Cicatrol, AntibioticeIasi, Romania). At five months the area of the right foot ulcer decreased and there were still 4 ulcers but just one with a diameter of 16mm. The pain disappeared (anamnestically) in 7 days –so it was maybe due to infection. Around the ulcerated areas reticulated atrophic hipopigmented areas were seen-atrophied blanche (Fig. 3). We noted also the disappearance of the livedoid area from the middle of the second toe finger. The perimaleolar foot ulcer was epithelized (Fig. 4). Wound cultures were negative. After another five months of continuous use of the topical cream the situation improves, the other three small ulcerations disappeared, the big one diminished at 12 mm but continues to stay on the right foot (Fig. 5).


DISCUSSIONS
Livedoid vasculopathy is a disease of the lower legs with painful chronic ulcerations and cutaneous atrophy blanche, it is hard to manage due to the resistance at topical and internal treatments and its potential to complicate with infections. Topical creams has sensitizing potential when used for long periods of time. The topical cream formula contains four active ingredients: Silversulfadiazine, bentonitehidrogel, chitosan and lactic acid.
Silver is used to reduce infections from ancient times. The use of silver impregnated dressings after laminectomies appear to limit/reduce the incidence of both postoperative deep and superficial wound infections [2]. The wide spectrum of antibacterial activity the low toxicity, minimal tissue reaction, ease of application suggest that topical silver sulfadiazine can safely be used in burns, surgical wounds and can be extended to other wound infections, wound covers and some transplant materials [3]. At the contact with the bacteria cell Ag + penetrates the bacterial membrane and stop the DNA synthesis so the bacteria cannot divide so it dies. Due to his redox potential Ag+ dissociate after the bacterialdestruction and acts in a bactericide manner ensuring a cyclic process. Silver sulfadiazine have excellent anti-bacterial activity and could be used initially while the identification of the infective agent is required for selecting the alternative topical agents and/or systemic therapy [4]. The second ingredient, bentonite is a clay which by absorbing or adsorbing moisture and impurities from the skin serve to cleanse and to refresh the surface of the skin surface and to aid the healing process. External use of Bentonite for wound healing is safe and feasible and the macroscopic healing of the wounds treated by Bentonite was superior versus control group [5]. The third ingredient is Chitosan- a polysaccharide obtained from crustaceans and with a regenerative effect on skin. Chitosan is a linear copolymer of B linked 2-acetamido-2 deoxy-B-D-glucopyranose and 2-amino-2-deoxy-B-Dglycopyranose, easily obtained by deacetilation of chitin, an abundant polysaccharide found in nature as a component of exoskeletons of crustaceans and insects. Topically used Chitosan bind on fibroblasts and stimulates the keratinocite proliferation and the repair of the epiderm [6]. Since its discovery approximately 220 years ago, Chitosan as a cationic natural polymer has been used as topical dressing in wound management owing to its hemostatic, stimulation of healing, antimicrobial, nontoxic, biocompatible and biodegradable properties [7]. It stimulates the imunocites and also leucocites, macrophages and fibroblasts [8], bloks nerve endings to reduce pain, absorbe fluids from inflammation, encourages natural blood clotting, forms barrier against infection, provides proteins for healing and scaffold for cell growth, strengthens new tissue, minimize scarring [9].
The protection of the host against bacterial infection is stimulated by chitosan. The effectiveness of chitosan bacteriastatic properties were tested against bacterial strains and a common skin fungus. Powered chitin, chitosan or whole crab shells were not effective in any of the tests, but solution of chitosan in acetic acid inhibited the bacterial strains and the fungus. The mechanism underlying the inhibition of bacterial growth, is though to be that the cationically charged amino-group may combine with anionic components such as N-acetylmuramic acid, sialic acid and neuraminic acid, on the cell surface, and may suppress bacterial growth by impairing the exchanges with the medium, chelating transition meal ions and inhibiting enzymes. Chitosan is characterized by high antibacterial and fungicidal activities [10]. The lactic acid is known as a antiwrinkle agent, hepls to the renewing of epiderma, stimulates the colagen sinthesis, ceramides and epidermal growing factor [11].
The associated Rosacea was not influenced by the evolution of the ulcers and i didn*#x2019;t find in literature the association with livedoid vasculopathy.
CONCLUSIONS
Livedoid vasculopathy is a disease of the lower legs with painful chronic ulcerations and cutaneous atrophy blanche. livedoid vasculopathy is a coagulation disorder. As a result, modern therapy strategies take into account to treat it with systemic anticoagulation. Topical therapies may be considered only as accompanying measures but very important.
It is hard to manage due to the resistance at topical and internal treatments-fibrinolitics, anticoagulants, anti-plateletagregants- and due it is potential to complicate with infections. Topical creams has sensitizing potential when used for long periods of time. The topical compound formula with four active ingredients: Silver sulfadiazine, bentonitehidrogel, chitosan and lactic acid it was a cheap treatment for the patient, it was tolerated without sensitizing even it was used continuously for 10 months. Unfortunately one ulcer didn’t close completely. Our experience was limited to one case of livedoid vasculopathy and of course more studies should be done in the future on this field.
AKNOWLEDGEMENTS
This paper is supported by the Sectoral Operational Programme Human Resources Development (SOP HRD), financed from the European Social Fund and by the Romanian Government under the contract POSDRU/159/1.5/S/137390.
Consent
The examination of the patient was conducted according to the Declaration of Helsinki principles.
REFERENCES
1. Trey Haunson G, David J, Prall N, Miller R, Livedoid Vasculopathy: Review of Pathogenesis, Clinical Presentation, Diagnostic Workup, and TreatmentCutis 2012; 90: 302-6.
2. Epstein NE, Do silver impregnated dressings materials limits infections after lumbar laminectomy with instrumented fusion?Surg Neurol 2007; 68: 483-5.discussion 485
3. Fox CL, JrTopical therapy and the development of silver sulfadiazineSurg Ginecol Obstet 1983; 157: 82-8.
4. Katara G, Chamania S, Chitnis S, Hemvani N, Chitnis V, Dahananjai SC, A comparative study of the effect of different topical agents on burn wound infectionsIndian J Plast Surg 2012; 45: 374-78.
5. Emami Razavi SH, Esmaeili N, Forouzania SK, Amanpour S, Rabbani S, Alizadeh AM, Effect of Bentonite on skin wound healing: experimental study in the rat modelActa Medica Iranica 2006; 44: 235-40.
6. Chatelet C, Damour O, Domard A, Influence of the degree of acetylation on some biological properties of chitosan filmsBiomaterials 2001; 22: 261-8.
7. Dai T, Tanaka M, Huang YY, Hamblin MR, Chitosan preparations for wound and burns: antimicrobial and wound healing effectsExpert Rev Anti Infect Ther 2011; 9: 857-9.
8. Aranaz I, Mengibar M, Harris R, Panos I, Miralles B, Acosta N, Galed G, Heras A, Functional Caracterisation of Chitin and ChitosanCurrent Chem Biol 2009; 3: 203-30.
9. Paul Wan, Sharma CP, Chitosan and Alginate Wound Dressings: A Short ReviewTrends Biomater Artif Organs 2004; 18: 18-23.
10. Balicka-Ramisz1 A, Wojtasz-Pajak A, Pilarczyk B, Ramisz1 A, Laurans1 L, Antibacterial anf antifungal activity of ChitosanISAH 2005 – Warsaw, Poland 2:
11. Kim SJ, Park JH, Kim DH, Won YH, Maibach HI, Increased in vivo collagen synthesis and in vitro cell proliferative effect of glycolic acidDermatol Surg 1998; 24: 1054-8.
Notes
Source of Support: European Social Fund and by the Romanian Government under the contract POSDRU/159/1.5/S/137390.
Conflict of Interest: None declared.
Comments are closed.