Parameatal urethral cyst of glans penis in children – A report of three cases
1Sudhaa Skin Centre, Jammu, India, 2Acharya Shri Chander College of Medical Sciences, Jammu, India
ABSTRACT
Parameatal urethral cysts are a rare benign condition usually seen in males. They are usually asymptomatic but may produce symptoms like difficulty in micturition, pain during intercourse, urinary retention and distortion of the urinary stream. We report three cases of parameatal urethral cyst in young males presenting as a spherical clear fluid filled cystic lesions over the external urethral meatus, causing distortion of the urinary stream and poor cosmesis. Histological examination of the excised cyst showed a monolocular cyst lined with pseudo-stratified epithelium with no evidence of inflammation. Complete surgical excision of the cysts was done and no recurrence was observed at follow-up.
Key words: Parameatal cyst; Glans penis cyst; External urethral meatus cyst
INTRODUCTION
Parameatal urethral cysts are a rare benign entity usually seen in males but rarely may be seen in females also. They were first described by Thompson and Lantin in 1956 and since then, around 50 cases have been reported in the literature [1,2]. These cysts are usually asymptomatic but may produce symptoms like difficulty in voiding, urinary retention, pain during intercourse or micturition, distorted urinary stream and poor cosmesis [2]. Herewith we report three cases of parameatal cyst in young males presenting with symptoms of distortion of urinary stream and poor cosmesis who were managed with complete cyst excision.
CASE REPORTS
Case 1
A 14 year old boy presented with a painless swelling over the glans penis which he noticed a year back. The swelling was asymptomatic in the beginning but for the last three months it was causing distortion of the urinary stream. There were no other symptoms other than distorted urinary stream and poor cosmesis. There was no history of trauma or application of topical medications. The boy gave history of needle aspiration of the lesion at some other centre six months back leading to its clearance at that time, but the lesion had recurred to its present size over the next six months. On examination, a smooth, spherical cystic mass about 0.8 cm in diameter was found at the external urethral meatus (Fig. 1). No inflammatory signs were present. On investigations, hematological counts, liver and renal function parameters were within normal limits. Urine microscopy and urine culture also revealed no abnormality. Complete excision of the cyst under local anesthesia was performed and good cosmetic results were obtained without any urinary flow problems. No recurrence was observed at six months of post-operative follow-up.

Case 2
A six year old male child presented to us with a three months history of a gradually progressive asymptomatic cystic swelling over the glans penis. There was no history of any preceding trauma or any surgical intervention. On examination, a well defined cystic swelling measuring 0.6cm in diameter was present over the glans penis without any inflammatory signs (Fig. 2). All the routine hematological and liver and renal function parameters were within normal range. Urine microscopy and urine culture also revealed no abnormality. From history and clinical examination a diagnosis of parameatal urethral cyst was made and complete excision of cyst under local anesthesia was done and no recurrence was observed over a post-operative follow-up period of eight months.

Case 3
A two year old child presented to us with an eight months history of development of an asymptomatic painless swelling over the glans. On examination, a well defined cystic swelling measuring 0.5 cm in diameter was present over the glans penis without any inflammatory signs. All the routine hematological and liver and renal function parameters were within normal range and urine microscopy and urine culture also revealed no abnormality. A diagnosis of parameatal urethral cyst was made a surgical deroofing of the cyst followed by phenolization of the cyst wall was done under general anesthesia and no recurrence was observed over a post-operative follow-up period of six months.
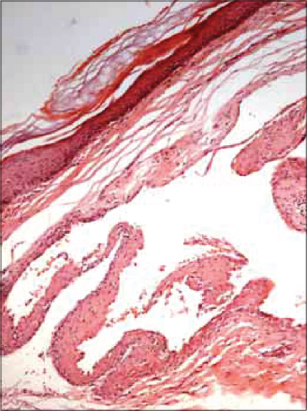
Histological examination of the excised cyst in both the cases showed a monolocular cyst lined with pseudo-stratified epithelium with no evidence of inflammation (Fig. 3).
DISCUSSION
Parameatal urethral cysts are a rare entity usually seen in boys but cases among females have also been reported [3]. Usually they appear spontaneously during the second decade of life but congenital and infantile onset has also been seen [2]. The etiology of parameatal cysts is still not completely understood. Obstruction of paraurethral ducts, either spontaneous or secondary to infection, has been postulated as one possible factor by a few authors while others believe that parameatal cysts occur in the process of delamination or separation of the foreskin from the glands [2]. Ichiyanagi et al [4] detected the presence of Prostate specific antigen (PSA) in the cells of parameatal cysts, thus giving credibility to hypothesis that these cysts originate from the accessory male sex glands in the penile urethra. Soyer et al [3] reported two cases of parameatal cysts in newborn females, which were associated with vaginal bleeding and breast enlargement, which point towards the possible role of estrogens in their development.
These cysts are usually small, measuring upto 1 cm in diameter. They usually occur on one side of the urinary meatus but bilateral cases have also been reported. Usually the parameatal cysts are asymptomatic but rarely may present with symptoms like difficulty in voiding, urinary retention, pain during intercourse or micturition, distorted urinary stream and poor cosmesis. If the cyst is traumatized, it may bleed, rupture or become infected [2].
Numerous treatment modalities like needle aspiration, marsupialisation, and decapping have been described in their management but complete surgical excision is the treatment of choice owing to lower chances of recurrence and better cosmetic results. Histologically, the cyst wall may be lined by columnar, squamous or transitional epithelium which varies according to the urethral segment of origin of the lesion [2,5].
In conclusion, a parameatal cyst is a benign, usually asymptomatic condition diagnosed on physical examination with a complete surgical excision providing good cosmetic results without recurrence.
CONSENT
The examination of the patient was conducted according to the Declaration of Helsinki principles.
REFERENCES
1. Lantin PM, Thompson IM, Parameatal cysts of the glans penisJ Urol 1956; 76: 753-5.
2. Lal S, Agarwal A, Parameatal Cyst: A Presentation of Rare Case and Review of LiteratureJ Clin Diag Res 2013; 7: 1757-8.
3. Soyer T, Aydemir E, Atmaca E, Paraurethral cysts in female newborns: role of maternal estrogenesJ Ped Adol Gyn 2007; 20: 249-51.
4. Ichiyanagi N, Shibata T, Matsumura T, Ishimoru H, Sakai I, Immunohistochemical identification of prostatic –specific antigen in parameatal urethral cysts of the glans penisBr J Urol 1998; 81: 170-1.
5. Aggarwal K, Gupta S, Jain VK, Goel A, Parameatal urethral cystIndian J Dermatol Venereol Leprol 2008; 74: 430.
Notes
Source of Support: Nil
Conflict of Interest: None declared.
Comments are closed.