Rare case report of mesenteric fibromatosis
Radhika Vidyasagar1, P. Sudarshan1, Sreedhar Suresh1, Vidya Bhat2, M. Subramanya2
1Department of General Surgery, MVJ Medical College, Bangalore, India, 2Department of Pathology, MVJ Medical College, Bangalore, India
ABSTRACT
Mesenteric fibromatosis is a part of the clinical-pathologic spectrum of deep fibromatoses. We report this rare case of primary mesenteric tumor that was diagnosed to be a mesenteric fibromatosis on histopathological examination. In majority of patients it may remain asymptomatic and the management of these tumors depends on histopathological examination. Postoperatively, patient was well and subsequent followup showed normal recovery.
Key words: Mesenteric cyst; Fibrzomatosis; Intra abdominal
INTRODUCTION
Mesenteric fibromatosis is a part of the clinical-pathologic spectrum of deep fibromatoses. The deep fibromatoses encompass a group of benign fibroproliferative processes that are locally aggressive and have the capacity to infiltrate or recur but not metastasize.
The deep fibromatoses are classified by anatomic location because they may arise from intra abdominal sites (mesenteric, pelvic, and retroperitoneal fibromatosis), the deep soft tissues of the abdominal wall (abdominal fibromatosis), and deep within extra abdominal soft tissues (extra abdominal fibromatosis).
Mesenteric fibromatosis occurs in a wide age range of patients, 14–75 years of age (mean, 41 years), and has no gender or race predilection.
Thirteen percent of patients with mesenteric fibromatosis have familial adenomatous polyposis (FAP), specifically, the Gardner syndrome variant of FAP. The small bowel mesentery is the most common site of origin of intraabdominal fibromatosis. We report this rare case of primary mesenteric tumor that was diagnosed to be a mesenteric fibromatosis on histopathological examination.
CASE REPORT
A 59-year-old male came to the surgery opd with complaints of pain abdomen since 1 month. On examination, his vitals were normal. On per abdomen examination, there was a solitary swelling measuring 15 × 12 cms, spherical, non tender, freely mobile with a band of resonance heard over the mass. A probable diagnosis of Mesenteric cyst was made.
INVESTIGATIONS
FNAC: Malignant Mesothelioma
Well-Differentiated Adenocarcinoma.
Ultrasound Abdomen and Pelvis
There is a large hyperechoic mass lesion measuring 11.5 × 14.9 × 16.5 cm arising from the Right Iliac Fossa (likely Caecum). There is increased vascularity within the lesion – likely GIST.
NCCT + CECT Abdomen
A well defined, large (measuring 15.6 × 11.3 × 17.5 cm) minimally enhancing, homogenous, solid mass lesion noted in the mesentery with adjacent distal ileal bowel wall thickening (6 mm), mesenteric fat stranding inferiorly, abutting and displacing the adjacent small bowel loops. The lesion is seen in the midline superiorly extending upto origin of SMA, inferiorly up to common iliac bifurcation, anteriorly abutting the anterior abdominal wall. The lesion is supplied by branches of SMA that are seen transversing through out the lesion.
Imp: Large, mesenteric mass lesion as described with adjacent ileal wall thickening – suggestive of GIST, likely to be arising from distal ileum.
PROCEDURE
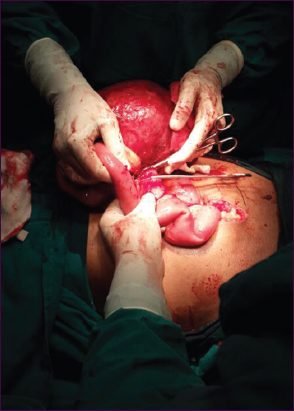
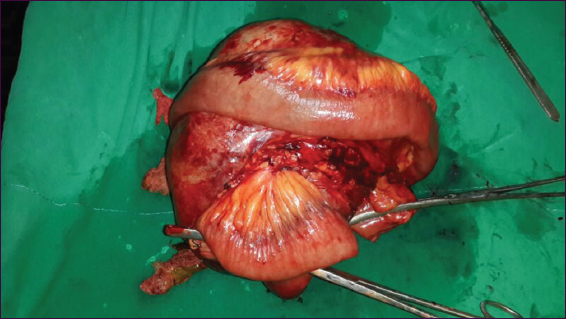
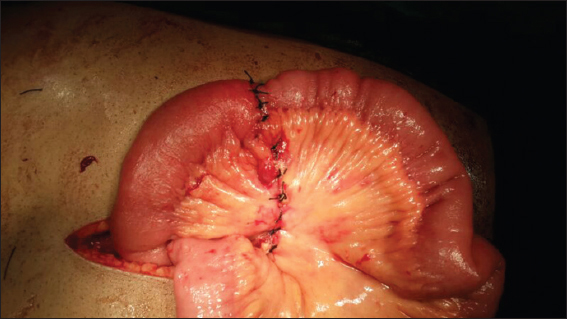
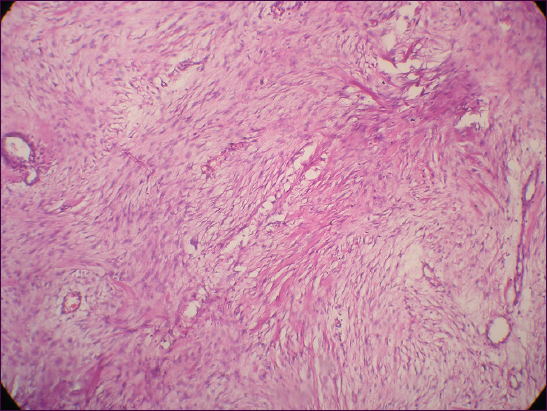
Patient underwent Exploratory Laparotomy with Intestinal resection and anastomosis under GA on 13/03/2014. A large, solitary mass was present at the root of the mesentery (Fig. 1) and adherent to recto sigmoid colon and small intestine (Fig. 2). Specimen weighed 2.4 kgs (Figs. 3 and 4 and was sent for HPE (Figs. 5 and 6).


Prior to the study, patient gave written consent to the examination and biopsy after having been informed about the procedure.
DISCUSSION
Mesenteric fibromatosis is a type of fibroblastic proliferation affecting the mesentery that develops usually as a consequence of surgical trauma, but it may occur spontaneously. It is sufficiently rare for no clear data of incidence and presented features to be known. The majority of patients with mesenteric fibromatosis remain clinically asymptomatic, with little or no focal symptoms until later in their course, at which stage they complain of abdominal pain and discomfort, constipation, vomiting, and organ compression symptoms, such as small bowel obstruction and hydronephrosis.
The etiology is unknown but an endocrine cause is suggested by: (i) the relative prevalence in perinatal women; (ii) tumour regression after the menopause; and (iii) regression with tamoxifen therapy [1].
As there is no classical symptomatology related to mesenteric fibromatosis, the diagnosis is confirmed only after the histological analysis of the tumor. Desmoid tumours are firm masses. On cross section these tumours are grayish and grossly homogenous.
Microscopically, mesenteric fibromatosis is characterized by a spatially homogenous proliferation of wavy spindle cells without atypia, associated with collagen among dilated vessels [2]. The mitotic count is relatively low with no evidence of necrosis and nuclear dedifferentiation.
The diagnosis of mesenteric fibromatosis is based on the microscopic examination and immunostaining. It is noteworthy that a CD117 antigen, expressed commonly in GISTs, can be positive in up to 75% cases of mesenteric fibromatosis. In contrast to GISTs, MF does not express CD34 and S100 protein. Recently, the expression of beta-catenin was revealed in fibromatoses that might prove helpful in the differential diagnosis in doubtful cases [3].
The sonographic features of mesenteric fibromatosis are nonspecific and chiefly dependent on collagen and fibroblast content and intralesional vascularity of the tumor. The results of the treatment might be biased due to the unpredictable course of this disease with some tumours regressing or remaining stable without any treatment.
The management of desmoids should be individualized and multimodal. The surgical resection should be performed only in localized tumours that do not invade the root of the mesentery. Intra-abdominal desmoids can be resected in 53–67% of cases. Fibromatoses are locally aggressive tumours that tend to recur when incompletely resected [4,5].
A high rate of recurrence after the surgical resection results from the incomplete resection, multicentric disease or surgical trauma as a new precipitating factor.
Radiotherapy may be used before surgery in cases of recurrence and inoperable lesions to shrink the tumor and make it operable. Adjuvant radiation therapy reduces recurrence of mesenteric fibromatosis to 20%–40%, compared to 40%–70% with resection only [5]. Recently, a successful therapy of a desmoid tumour resistant to traditional chemotherapeutic regimens was reported with imatinib, a tyrosine kinase inhibitor that is successfully used in advanced gastrointestinal stromal tumours.
CONCLUSION
Mesenteric fibromatosis is a rare tumour that in majority of patients may remain asymptomatic and the management of these tumors depends on histopathological examination.
Consent
The examination of the patient was conducted according to the Declaration of Helsinki principles.
REFERENCES
1. Kempson RL, Fletcher CD, Evans HL, Hendrickson MR, Sibley RK, Tumors of the Soft Tissues 1998; Washington, DC, USA: Armed Forces Institute of Pathology;
2. Lotfi AM, Dozois RR, Gordon H, Hruska LS, Weiland LH, Carryer PW, Mesenteric fibromatosis complicating familial adenomatous polyposis: predisposing factors and results of treatmentInt J Colorectal Dis 1989; 4: 30-6.
3. Ko SF, Lin JW, Ng SH, Huang CC, Wan YL, Huang HY, Spontaneous isolated mesenteric fibromatosis: sonographic and computed tomographic findings with pathologic correlationUltrasound Med Biol 2006; 32: 1141-9.
4. Burke AP, Sobin LH, Shekitka KM, Federspiel BH, Helwig EB, Intra-abdominal fibromatosis. a pathologic analysis of 130 tumors with comparison of clinical subgroupsAm J Surg Pathol 1990; 14: 335-41.
5. Levy AD, Rimola J, Mehrotra AK, Sobin LH, From the archives of the AFIP: benign fibrous tumors and tumorlike lesions of the mesentery: radiologicpathologic correlationRadiographics 2006; 26: 245-64.
Notes
Source of Support: Nil
Conflict of Interest: None declared.
Comments are closed.