Comparison between the effects of Daivonex cream alone and its combination with narrowband ultraviolet B in treatment of psoriasis
Shahla Babaei Nejad, Hamideh Herizchi Ghadim, Abolfazl Ezzati, Sina Nobahari, Esmail Emami Khatib, Sima Masoudnia
Department of Dermatology, Sina Hospital, Faculty of Medicine, Tabriz University of Medical Sciences, Tabriz, Iran
ABSTRACT
Introduction: Psoriasis is a chronic immune disorder that multiple factors are involved in its creation. Psoriasis is not curable but a large number of local and systemic treatments for psoriasis are available that can reduce symptoms and recurrence of the disease. Treatment is selected based on severity of illness, associated comorbidities, patient preference[including costs and convenience], and evaluation of the effectiveness of patient response to treatment.
Methods: 94 cases included from patients admitted to the Sina dermatology clinic with diagnosis of psoriasis. They were randomly divided in two groups. First group treated with Calcipotriol alone while the second group treated with calcipotriol and NBUVB phototherapy.
Results: According to the results of our study the subjects in the two groups in terms of sex, age, weight, height, history of systemic disease, duration of psoriasis, site of involvement and the extent of the lesions were not significantly differ. An average improvement in lesion thickness, erythema and scaling and investment, and improve overall recovery of waste per week in the fourth, eighth and twelfth week after treatment, In the second group were significantly higher than the first group.
Conclusion: Daivonex cream in combination with NBUVB phototherapy has a faster and more recovery in a given time. Daivonex with NBUVB phototherapy can be used to provide better results.
Key words: Psoriasis; Daivonex cream; NBUVB phototherapy
INTRODUCTION
Psoriasis is a chronic, relapsing inflammatory skin disease with silver plaques, Shell transition, and erythematous condition. Psoriasis is a polygenic disease that can occur at any age. Although in more than 75% of patients, the first symptoms are manifested before the age of 40 [1,2]. Furthermore, the association between psoriasis and inflammatory and metabolic disorders have also been reported. Several factors are involved in causing psoriasis such as trauma, infections, lifestyle, such as obesity, smoking and certain medications such as beta-blockers, and lithium, antimalarial drugs [3], nonsteroidal anti-inflammatory drugs, also Corticosteroid dose reduction noted in people who are genetically prone to cause disease [4,5].
From NBUBV In combination with Calcipotriol is also used to treat psoriasis. Studies that have evaluated the combined effect of Calcipotriol and NBUBV have offered varying results [6,7]. In this study, we attempt to evaluate the effectiveness of the cream Daivonex alone and to combine this method with phototherapy with NBUBV and to Choose an appropriate method that can, cause the greatest improvement in shortest time And can be more effective and safe therapy for the treatment of these patients.
METHODS AND MATERIALS
All the patients referred to the dermatology department of the sina hospital from October 2013 to March 2014 witch had been diagnosed with psoriasis, we chose the study cases totally random. To determine the sample size we used Rim Jh and colleagues study. In this study, the changes in the intensity of the thickness (induration) was considered as the primary outcome 94 individuals.
During the process of collecting samples from individuals who have less than 10% BSA or had limited psoriasis, if other criteria were matched they referred to responsible resident to be reviewed. The patients were randomly divided into 2 groups of 47, with no age limit. Anthropometric characteristics such as height and weight were determined for each individual. Duration of illness in patients was determined and patients were categorized according to the type of medication or unit weight in mg doses and duration of drug use. And each group was been treated with one of the 2 therapy methods as follows: All the patients underwent routine tests before starting treatment. Those in the treatment group of Daivonex.
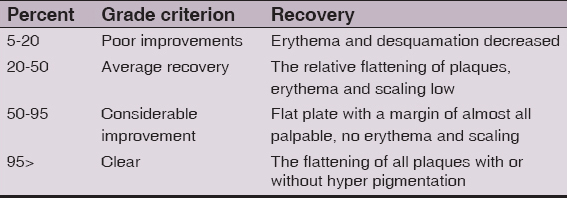
Cream used 5.0 mg every 12 hours to the surface of the body used the palm of a hand to measure it. Patients used creams with Behestan Behdasht (under license Leo pharma, Denmark) brand. Those in the treatment group witch treated with cream Daivonex with NBUVB 2 times a week using Dermapal 800 Davlin machine made in United States of America with a primary energy of 2.0 joules per square centimeter were under phototherapy. In the next sessions 1/0 joules per square centimeter on the amount of energy was added by the system. These patients were similar to the previous group witch were using cream with the difference that in the days of phototherapy, the cream used after PHOTOTHERAPY. All patients at baseline and 4, 8 and 12 weeks after starting treatment were visited and the improvement of erythema, scaling, thickening (induration) lesion (no = 0, less than 30% = low, 30 -60% = average, over 60% = high) and the response to treatment was assessed and defined in to grades according to the following Table 1.
Table 1: Grades evaluation of treatment
For 12 weeks, according to previous studies, it was enough for patients and patients relapse after completion of the study were not examined.
To eliminate bias in the study some inclusion criteria were determined.
Inclusion criteria for this study include:
- Having mild psoriasis
- The non-glare
- No other systemic diseases
- Lack of lupus erythematous or derma Pygmantvzvm
- No history of melanoma
- No other skin malignancies
- Arsenic consumption
- Pregnant women or lactation
- Willingness to participate in the study
- Do not use other treatments in the last month.
Exclusion criteria:
Failure to comply with any of the criteria for inclusion
This study is registered with registration number IRCT138903294207N1 in database of registered clinical trials.
Findings
In this study 85 patients, 47 males (55.3%) and 38 females (44.7 %) participated. 24 males (55.8%) and 19 women (44.2%) participated in group A treated with Daivonex cream alone, 23 men (54.8%) and 19 females (45.2%) participated in group B treated with Daivonex cream and ultra-violet with narrow band B (NBVUB), the frequency of sex differences in the two groups was not statistically significant (P=0.923).
The duration of the disease, patients in group A, with an average 4.16±4.45 years and group B with an average of 5.37±7.82 years. Statistically significant differences between the groups in duration of disease was observed (P=0.387).
Among the most affected areas of the body, legs. Statistically no significant differences showed in the place of the lesions between the two groups (P=0.594).
Due to the significant chi-square value of P=0.842, there is no significant difference in the extent of lesions between the two groups.
According to the results presented by sex, age, weight, height, history of diabetes, duration of psoriasis, the involvement of problem and size difference between the two groups A and B was not significant. In comparing the recovery of patients in groups A and B, of erythema, scaling and thickness investment (induration) at weeks 4, 8 and 12, the following information was obtained:
About Improving in the levels of erythema 4 grades including, no erythema = 4, (low) less than 30% = 3, (average) 30-60% = 2 and (much) more than 60% = 1, coded and measured.
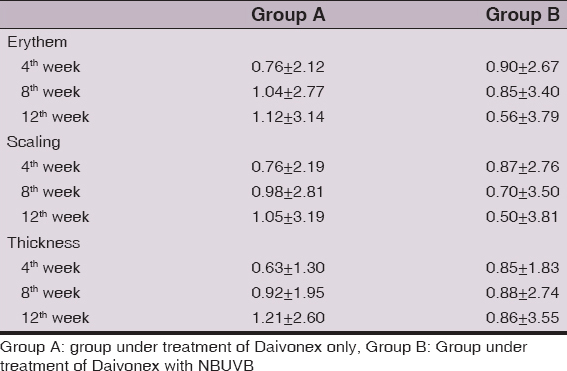
All patients in both groups at baseline were with high erythema (60%). The mean improvement in erythema at different is described weeks inTable 2.
Table 2: Frequency of results of two group treatment
About Improve in the investment of Scaling, 4 grades including, no scaling = 4, (low) less than 30% = 3, (average) 30-60% = 2, and (much) more than 60% = 1 encoded and measured.
All patients in both groups at baseline had more scaling investment. The mean improvement in the scaling investment (Table 2) is visible. In group B recovery were greater and faster than in group A.
About Improving in thickness (induration) four levels including, no abnormal thickness = 4, (low) less than 30% = 3, (average) 30-60% = 2 and (much) more than 60% = 1 encoding and measured.
In All patients of both groups at baseline lesions were too thick. Average improvement in thickness described in Table 1. Five levels in recovery including: no recovery = 0, low recovery in scaling or erythema less than 20% = 1, average recovery with smooth scaling and erythema (20-50%) = 2, nice smooth complete recovery with a palpable edge of the crust and no erythema (50-95%) = 3 and full recovery (over 95%) = 4 is defined and measured.
Improvement Process at week 4 in Group A was 1.19± 0.76 and in group B was 1.76±0.93. Due to the significant level of p=0.002 in the recovery of group A and B at 4 weeks of treatment, there was a statistically significant difference.
In group A, the mean recovery in week 8 was 1.86±1.06 and in group B was 2.71± 0.94. Due to the significant level of P=0.000 in the recovery of group A and B at 8 weeks of treatment, there was a statistically significant difference.
In group A, the mean recovery in week 12 was 2.56±1.18 and in the group B was 0.86 ± 3.55. Due to the significant level of P=0.000 in the recovery of group A and B at 12 weeks of treatment, there was a statistically significant difference.
In both groups recovery was observed but in group B recovery was more and faster than in group A. So that at the end of the study the group witch used cream Daivonex had 30.2% of complete recovery but patients in group B witch treated by phototherapy with narrowband ultra violet and Daivonex cream in the combination 73.8% of complete recovery was observed.
DISCUSSION
According to the results of our study subjects in the two groups in terms of sex, age, weight, height, history of diabetes, duration of psoriasis, the plight and size differences were not significant The mean improvement in erythema and crust investment and improve in lesion thickness overall recovery of lesion in the fourth week, eighth and twelfth after starting treatment in patients who were treated with creams and phototherapy were Significantly higher than the group that used the cream alone. The results of our study show that the use of cream in combination with phototherapy Daivonex Phototherapy with faster and more recovery at a time can be used to provide better results [8]. It can be concluded that patients can improve the speed of treatment side effects, including cumulative effects of phototherapy dose reduction That the matter should be further investigated in other comparative studies. Similar to Noborio et al study in 2006 concluded that the therapeutic effects of Calcipotriol is higher than other drugs in combination with phototherapy [9]. The results of our study showed that Calcipotriol in combination with phototherapy increase the speed and the amount of improvement.
As a study done by Jong-Hyun Rim et al [10] in our study, the use of Calcipotriol cream in combination with phototherapy with an appropriate treatment was introduced to accelerate and enhance recovery.
As a study done by Takahashi et al [6], the results of our study showed that the combination of Calcipotriol Ointment with NB-UVB twice a week, compared to other treatments, the rate and extent of psoriasis of lesion can be further improved.
As a study done by Rogalski et al [7] as well as a study done by Roussaki-Schulze et al [11], in our study group Calcipotriol alone received less improvement than the other groups showed. This could indicate an increased therapeutic effect in combination with other treatments is Calcipotriol, or excimer laser, or narrowband ultraviolet radiation.
Unlike our study Karakawa et al as “the period of remission treated with narrowband ultraviolet B in psoriasis vulgaris” did And retrospectively studied the factors that influence the duration of remission after photo chemotherapy so we compared [8]. The two methods together, to achieve a therapeutic effect that is the most efficient and lowest paid.
CONCLUSION
The results of our study show that the use of cream Daivonex in combination with phototherapy By creating more and faster recovery time can be as a treatment that can be used to provide better results So that in the group treated with cream Daivonex, at the end of the study 30.2% of patients achieved complete remission, while the combination of cream and ultra violet Daivonex narrowband cure rate was 73.8 percent.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Statement of Informed Consent
Informed consent was obtained from all patients for being included in the study.
REFERENCES
1. Kaur J, Shrama VK, Sethuraman G, Tejasvi T, Comparison of the efficacy of psoralen ultraviolet A with narrowband ultraviolet B phototherapy for the treatment of chronic plaque psoriasis in patients with skin types 4 and 5Clin Exp Dermatol 2008; 33: 513-5.
2. Seckin D, Usta I, Yazici Z, Senol A, Topical 8- methoxypsoralen increases the efficacy of narrowband ultraviolet B in psoriasisPhotodermatol Photoimmunol Photomed 2009; 25: 237-41.
3. Asawanonda P, Amornpinyokeit N, Nimnuan C, Topical 8-methoxypsoralen enhances the therapeutic results of targeted narrowband ultraviolet B phototherapy for plaque-type psoriasisJ Eur Acad Dermatol Venereol 2008; 22: 50-5.
4. Menter A, Korman NJ, Elmets CA, Feldman SR, Gelfand JM, Gordon KB, Guidelines of care for the management of psoriasis and psoriatic arthritis. Section 5. Guidelines of care for the treatment of psoriasis with phototherapy and photochemotherapyJ Am Acad Dermatol 2009; 62: 114-35.
5. Kleinpenning MM, Smits T, Boezeman J, van de Kerkhof PC, Evers AW, Gerritsen MJ, Narrowband ultraviolet B therapy in psoriasis: randomized double blind comparison of high- dose and low- dose regimensBr J Dermatol 2009; 161: 1351-56.
6. Takahashi H, Tsuji H, Ishida-Yamamoto A, Iizuka H, Comparison of clinical effects of psoriasis treatment regimens among calcipotriol alone, narrowband ultraviolet B phototherapy alone, combination of calcipotriol and narrowband ultraviolet B phototherapy once a week, and combination of calcipotriol and narrowband ultraviolet B phototherapy more than twice a weekJ Dermatol 2013; 40: 424-7.
7. Rogalski C, Grunewald S, Schetschorke M, Bodendorf MO, Kauer F, Simon JC, Treatment of plaque-type psoriasis with the 308 nm excimer laser in combination with dithranol or calcipotriolInt J Hyperthermia 2012; 28: 184-90.
8. Karakawa M, Komine M, Takekoshi T, Sakurai N, Minatani Y, Tada Y, Duration of remission period of narrowband ultraviolet B therapy on psoriasis vulgarisJ Dermatol 2011; 38: 655-60.
9. Noborio R KK, Shintani Y, Morita A, Comparison of the efficacy of calcipotriol and maxacalcitol in combination with narrow band ultraviolet B therapy for the treatment of psoriasisJ Dermatol 2006; 375: 84-118.
10. Rim JH, Choe YB, Youn JI, Positive effect of using calcipotriol ointment with narrow-band ultraviolet B phototherapy in psoriatic patientsPhotodermatol Photoimmunol Photomed 2002; 18: 131-4.
11. Roussaki-Schulze A, Kouskoukis C, Klimi E, Zafiriou E, Galanos A, Rallis E, Calcipotriol monotherapy versus calcipotriol plus UVA1 versus calcipotriol plus narrow-band UVB in the treatment of psoriasisDrugs Exp Clin Res 2004; 31: 169-74.
Notes
Source of Support: Nil,
Conflict of Interest: None declared.
Comments are closed.