Superficial thrombophlebitis mimicking cutaneous polyarteritis nodosa as an early and sole cutaneous manifestation of Behçet’s disease
Tomoko Hiraiwa, Toshiyuki Yamamoto
Department of Dermatology, Fukushima Medical University, Fukushima 960-1295, Japan
Sir,
A 32-year-old woman presented to us with multiple painful nodules and erythema on her ankles which had appeared two weeks previously. She had a mild fever for previous half a year and experienced blurred vision and conjunctival hyperemia for a month, which was diagnosed as iridocyclitis. On physical examination, her ankles were swollen and tender, and irregularly-shaped erythema with unclear borders was observed (Fig. 1). Laboratory findings revealed leukocytosis in her peripheral blood and a slightly increased C-reactive protein level (5.3 mg/dl). Myeloperoxidase-anti-neutrophil cytoplasmic antibody (MPO-ANCA), proteinase-3 (PR3)–ANCA, and antiphospholipid antibody were all negative. Histological examination of the erythema revealed a thrombus of a subcutaneous vessel (Fig. 2) along with dense infiltration of neutrophils, lymphocytes and their nuclear dust in the vessel wall and deposition of fibrin on the wall as well as diapedesis of red blood cells (Fig. 3). Both Elastica-Masson and Elastica–van Gieson staining showed signs of non-circumferential single-layered elastic fibers along the inner cavity of the vessel and intravascular lumen being compressed (Fig. 4). Later, we interviewed her in detail and found that she often got aphthous stomatitis. We made a conclusive diagnosis of incomplete-type Behçet’s disease.

Figure 1: Irregularly shaped erythema with unclear borders on the ankles.

Figure 2: A thrombus of a subcutaneous vessel.
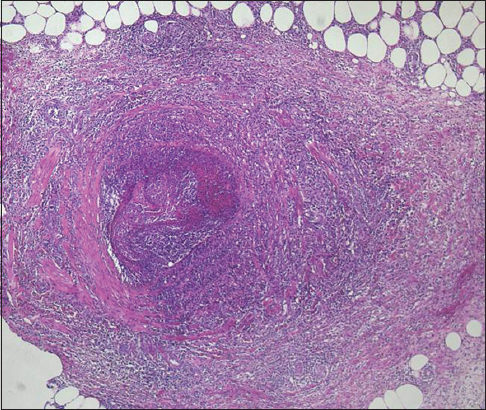
Figure 3: Infiltration of neutrophils, lymphocytes and their nuclear dust in the vessel wall with deposition of fibrin on the wall as well as diapedesis of red blood cells.
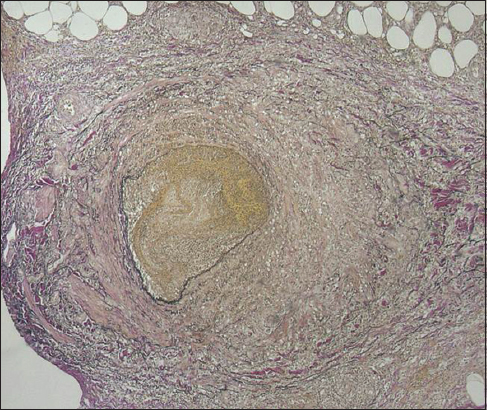
Figure 4: Non-circumferential single-layered elastic fibers along the inner cavity of the vessel and compressed intravascular lumen was revealed by Elastica-Masson and Elastica–van Gieson staining.
Prior to the study, patient gave written consent to the examination and biopsy after having been informed about the procedure.
Our case presented with multiple painful nodules on the bilateral lower limbs. At first, we clinically diagnosed her as having cutaneous polyarteritis nodosa (cPN), and histological features were suggestive of vasculitis.
However, detailed examination revealed a thrombus with severe perivascular infiltration of inflammatory cells in the subcutis, and Elastica–van Gieson staining detected concentric bundles of elastic fibers between smooth muscles in veins. Prior to the onset of the cutaneous lesions, the patient had been diagnosed as having iridocyclitis. Thrombophlebitis was observed as the sole cutaneous sign, unaccompanied by aphthae, erythema nodosum, or folliculitis. Thus, we diagnosed our patient as having incomplete-type Behçet’s disease.
Thrombophlebitis sometimes mimics cPN not only clinically but also histologically and is therefore easily misdiagnosed as cPN [1,2]. Chen [3] reported the main reasons for misdiagnosis, i.e. i) subcutaneous veins in the lower legs have a thick muscular layer that resembles that of the muscular veins, ii) tissue sections obtained vertically show a concentric muscular layer with a round luminal appearance, which resembles an internal elastic lamina in the muscular layer of the arteries, and iii) subcutaneous veins in the lower legs reveal intimal elastic fiber proliferation, resembling that of the arteries. Although the differential diagnosis is sometimes difficult, thrombophlebitis should be considered when diagnosing cPN in order to avoid misdiagnosis and overtreatment.
CONSENT
The examination of the patient was conducted according to the Declaration of Helsinki principles.
REFERENCES
1. Vikas A, Atul S, Singh R, Sarbmeet L, Mohan H, Behçet disease with relapsing cutaneous polyarteritis nodosa-like lesions, responsive to oral cyclosporine therapyDermatol Online J 2003; 9: 9
2. Heller M, Behçet disease (incomplete) and cutaneous polyarteritis nodosaDermatol Online J 2005; 11: 25
3. Chen KR, The misdiagnosis of superficial thrombophlebitis as cutaneous polyarteritis nodosa: features of the internal elastic lamina and the compact concentric muscular layer as diagnostic pitfallsAm J Dermatopathol 2010; 32: 688-93.
Notes
Source of Support: Nil,
Conflict of Interest: None declared.
Comments are closed.