A tricky man issue: Angiokeratomas of scroti
Yugandar Inakanti1, Thimmasarthi Venkata Narsimha Rao2
1Department of Dermatology Venerology and Leprosy, P.E.S. Institute of Medical Sciences and Research, Kuppam -517425, Chittoor District, Andhra Pradesh, India, 2Department of Dermatology Venerology, Guntur Medical College, Guntur, Andhra Pradesh, India
ABSTRACT
Angiokeratoma is a benign cutaneous lesion of capillaries, resulting in small marks of red to blue colour spots and characterized by hyperkeratosis. They often unnoticed, may become crusty and bleed if accidentally scratched or damaged.
We presented our cases because of its apprehension, health anxiety created to patients by complaint it as malignancy of scrotum and sexually transmitted diseases. Most of patients seek medical advice to rule out sexually transmitted diseases and malignancy. The cases well highlights these unusual complaints of Angiokeratoma and only two reports of multiple Angiokeratomas available in an Indian Dermatology literature.
Key words: Angiokeratoma; Electrocauterisation; Histopathology; Laser; Scrotal Bleeding; Vascular malformation
INTRODUCTION
Angiokeratoma of the Scroti is often a benign and asymptomatic condition [1]. It is a vascular dermatosis characterised by dilated vessels of the superficial dermis associated with epidermal hyperplasia. Angiokeratomas are characterized by ectasia of the superficial dermal vessels and hyperkeratosis of the overlying epidermis.
The term ‘Angiokeratoma’ is derived from three Greek words meaning vessels, horn and tumour respectively, although it is not a tumour in its true sense. In 1896, John Addison Fordyce [2] reported the first case of atypical Angiokeratoma of scrotum followed by Imperial and Helwig [3] in 1967.
We presented our cases because of its apprehension, health anxiety created to patients by complaint it as malignancy of scrotum and sexually transmitted diseases. Most of patients seek medical advice to rule out sexually transmitted diseases and malignancy. The cases well highlights these unusual complaints of Angiokeratoma and only two reports of multiple Angiokeratomas available in Indian literature. The clinical and histological features of this cases are described here.
CASE REPORT
Case 1
A 26 year old male patient reported to our department with a one month history of multiple bleeding spots over the scrotum after sexual intercourse. He was openly worried about the possibility of a sexually transmitted infection and denied any urethral discharge, dysuria or sexual dysfunction (Fig. 1).

Case 2
A 31 years male patient working as daily labourer came with chief complaints of severe itching over scrotum since 6 months (Fig. 2).

Case 3
A 17 years boy was presented with complaints of red spots over scrotum since 6 months (Fig. 3).

Case 4
A 28 years old male complaints of black spots over scrotum since one year (Fig. 4).

They had no prior medical history and were not taking any regular medication. No history of similar skin lesion in family members. They had no history of systemic complaints. The physical examinations were within normal limits. Palpation ruled out varicocele, epididymal mass or inguinal hernia.
On cutaneous examination, there were multiple purple to black colour, diffusely distributed, dome shaped papules over scrotum, size of 2-6 mm, few lesions show scaling. Hair, nail and oral mucosa were not involved.
Laboratory investigations revealed normal Complete blood counts, ESR, Liver function tests and Kidney function tests. Screening for HIV, Hepatitis B, and Hepatitis C were Negative. VDRL was Non reactive. Radiography of the chest and vertebral column, as well as abdominal sonography was normal. USG abdomen, pelvis and scrotum were done to rule out any vascular anomaly.
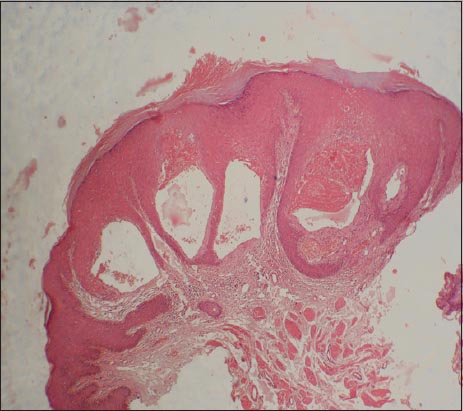
Histopathological examination from one of the papules on skin under haematoxylin and eosin staining (H & E) showed mild hyperkeratosis with hyper plastic epidermis and elongated rete ridges encircling large, numerous, dilated, congested capillaries filled with RBC’s in an expanded papillary dermis (Figs 5 and 6). On the basis of clinical features and histopathology, the patient was diagnosed as Angiokeratoma of Fordyce.

The patient’s informed consent was obtained.
Prior to the study, patient gave written consent to the examination and biopsy after having been informed about the procedure
DISCUSSION
Angiokeratomas are well-circumscribed vascular lesions consisting of superficial vascular ectasia and hyperkeratosis. Angiokeratomas result from ectatic dilation of pre-existing vessels in the papillary dermis.
Five variants of angiokeratomas have been recognized:
- Angiokeratoma of the scrotum or vulva (Fordyce type);
- Solitary or multiple papular angiokeratoma;
- Mibelli angiokeratoma;
- Angiokeratoma circumscriptum;
- Angiokeratoma corporis diffusum;
The onset is usually in the second or third decade mostly after the age of 40 years. The prevalence is reported to increase with age, from 0.6% in 16-year-old males to 17% in those older than 70 years. No familial inheritance.
The etiology is unknown. Local venous hypertension might play a causative role and it is more common in patients with coexisting varicocele, hydrocele, inguinal hernia, benign prostatic hypertrophy, or haemorrhoid [4]. Some authors described it as a degenerative disorder [5]. Some experts thought to result from injury or trauma to or chronic irritation of the wall of a venule in the papillary dermis.
Angiokeratoma of Fordyce is the most common type of Angiokeratoma, commonly seen over the scrotum, can also be seen on the vulv, labia majora, clitori and thighs. Occasionally over the penile shaft and glanspenis [6]. Vulvar lesions may be associated with vulvar varicosities, haemorrhoids, oral contraceptive pills or increased venous pressure during pregnancy.
Fordyce angiokeratoma classically presents as multiple dark red, dome-shaped papules of 2 to 6 mm in diameter, with a discrete keratotic surface. Keratotic part may be involuntarily scratched off to produce considerable bleeding. Lesions of recent onset are red, soft, and compressible, whereas older lesions are dark blue to purple, firm, and non compressible. Solitary lesions may confuse with melanoma due to their black colour.
Angiokeratoma of the scrotum can lead to diffuse redness of the scrotum [7]. Angiokeratoma show steaks or bands of papules due to linear distribution, rough scaling on the surface and blood blisters are also experienced sometimes. The lesions can cause the patient health anxiety and embarrassment.
In Differential diagnosis Cherry Hemangioma, Granuloma pyogenicum, Malignant Melanoma, Melanocytic Naevi, Petechial angioma, Genital warts and Angiokeratoma Corporis Diffusum (Fabry Syndrome).
Histopathogy of Angiokeratomas shows mild hyperkeratosis and elongated rete ridges encircling large, numerous, dilated vessels filled with thrombi in the papillary dermis. There are many communicating lacunae in the sub papillary layer are lined with endothelium and connected underneath by dilated veins.
Our cases show mild hyperkeratosis with hyper plastic epidermis and elongated rete ridges encircling large, numerous, dilated, congested capillaries filled with RBC’s in an expanded papillary dermis. So Diagnosis is confirmed.
Most of Angiokeratomas are benign and treatment is generally unnecessary. The Primary therapy is Reassurance. If treatment needed local destructive methods like electrodessication, cryotherapy, lasers therapy like Pulsed dye laser [8] and Erbium: YAG [9] lasers and excision may be considered for symptomatic lesions or for cosmoses. Our patients undergone for Electrodessication and advised follows up after three months for recurrence and cosmetic problems.
CONCLUSION
Angiokeratomas are hyperkeratotic vascular cutaneous lesions which may be localized or diffuse. The major morbidity comes from bleeding, anxiety and sometimes over-treatment due to misdiagnosis. Usually, they do not require treatment. Reassurance is the prime therapy. If treatment is needed, laser, electrocoagulation, excision, or cryotherapy may be used.
In conclusion, there have been only a few reports about Angiokeratoma of Scroti in the dermatologic literature. Pahwa P, et al. reported a case of Punctate vascular papules on the tongue and scrotum [10]. Ghosh SK, et al. reported a case of Acute scrotal bleeding [11]. Masuria BL, et al. also described an Angiokeratoma of Fordyce on unusual site [12]. Pande, et al. reported a case of Unilateral Angiokeratoma of fordyce [13], to the best of our knowledge, we are reporting four cases of multiple Angiokeratomas of scrotum. So we suggest that the title name Fortuitous stain – A Tricky man issue: Angiokeratomas of Scroti.
ACKNOWLEDGEMENT
- Dr Shiva Kumar, Prof & HOD, Department of DVL, Pesimsr, Kuppam.
- Dr Krishna H.L, Principal, PES Medical College, Kuppam.
CONSENT
The examination of the patient was conducted according to the Declaration of Helsinki principles. Written informed consent was obtained from the patient for publication of this article.
REFERENCES
1. Trickett R, Dowd H, Angiokeratoma of the scrotum: a case of scrotal bleedingEmerg Med J 2006; 23: 5-7.
2. Fordyce JA, Angiokeratoma of the scrotumJ Cutan Genitourin Dis 1896; 14: 81-7.
3. Imperial R, Helwig EB, Angiokeratoma. A clinicopathological studyArch Dermatol 1967; 95: 166-75.
4. Erkek E, Basar MM, Bagci Y, Karaduman A, Bilen CY, Gokoz A, Fordyce angiokeratomas as clues to local venous hypertensionArch Dermatol 2005; 141: 1325-6.
5. Shahidullah H, Moss C, Burns T, Breathnach S, Cox N, Griffiths C, Angiokeratoma of the scrotumRook’s Textbook of Dermatology 2010; 8th ed. Wiley-Blackwell; 18.58-18.60.
6. Bechara FG, Huesmann M, Stücker M, Altmeyer P, Jansen T, An exceptional localization of angiokeratoma of Fordyce on the glans penisDermatology 2002; 205: 187-8.
7. Miller C, James WD, Angiokeratoma of Fordyce as a cause of red scrotumCutis 2002; 69: 50-1.
8. Bechara FG, Jansen T, Wilmert M, Altmeyer P, Hoffmann K, Angiokeratoma Fordyce of the glans penis: combined treatment with erbium: YAG and 523 nm KTP (frequency doubled neodynium: YAG) laserJ Dermatol 2004; 31: 943-5.
9. Lapidoth M, Ad-El D, David M, Azaria R, Treatment of angiokeratoma of Fordyce with pulsed dye laserDermatol Surg 2006; 32: 1147-50.
10. Pahwa P, Meena D, Tanveer N, Sharma VK, Sethuraman G, Punctate vascular papules on the tongue and scrotumIndian J Dermatol 2012; 57: 228-9.
11. Ghosh SK, Bandyopadhyay D, Acute scrotal bleedingJ Emerg Trauma Shock 2010; 3: 416-7.
12. Masuria BL, Gupta LK, Batra A, Kothiwala RK, Singh MK, Angiokeratoma of fordyce on unusual siteIndian J Dermatol Venereol Leprol 1999; 65: 240-1.
13. Pande SY, Kharkar VD, Mahajan S, Unilateral Angiokeratoma of FordyceIndian J Dermatol Venereol Leprol 2004; 70: 377-9.
Notes
Source of Support: Nil
Conflict of Interest: None declared.
Comments are closed.