DOI: 10.7241/ourd.20123.48 article in PDF
Our Dermatol Online. 2012; 3(3): 212-214
Date of submission: 28.03.2012 / acceptance: 28.04.2012
Conflicts of interest: None
SUCCESSFUL TREATMENT OF INFUNDIBULOFOLLICULITIS WITH TOPICAL TRETINOIN. REPORT OF A CASE
Seema Srinivasa, Metikurke Vijayashankar
MVJ Medical College and Research Hospital, Bangalore, India
Corresponding author: Dr. Seema Srinivasa e-mail:seem.srnvs@gmail.com
How to cite an article: Srinivasa S, Vijayashankar M. Successful treatment of infundibulofolliculitis with topical tretinoin. Report of a caseu. Our Dermatol Online 2012; 3(3): 212-214.
Abstract
First described in 1968 by Hitch and Lund. Disseminated and Recurrent infundibulofolliculitis (DRIF) is an uncommon eruption characterized by recurrent, pruritic follicular papules commonly seen on the trunk and proximal extremities. Rarely limited to the neck. It is much more common in black population but has also been reported in other ethnicities including Caucasians. Its etiology has constantly been debated with a few authors describing it as a variant of atopic dermatitis while others have refuted the same as a family history of atopy is not present. Various others have classified DRIF as variants of follicular eczema, along with lichen spinulosus and juxtaclavicular beaded lines. Its treatment also varies with different authors claiming response to steroids, isotretinoin, UVA therapy, keratolytics and tetracyclines. We describe a case of localized infundibulofolliculitis of the neck diagnosed in a 21 year old female who was successfully treated with a course of topical tretinoin 0.025%. The presenting history, clinical findings, biopsy results and available literature are reviewed.
Key words: infundibulofolliculitis; neck; Caucasians; female
Introduction
First described in 1968 by Hitch and Lund [1]. Disseminated and Recurrent infundibulofolliculitis (DRIF) is an uncommon eruption characterized by recurrent, pruritic follicular papules commonly seen on the trunk and proximal extremities. Rarely limited to the neck [2]. It is much more common in black population [3] but has also been reported in other ethnicities including Caucasians [4]. Its etiology has constantly been debated with a few authors describing it as a variant of atopic dermatitis [5] while others have refuted the same [6] as a family history of atopy is not present. Various others have classified DRIF as variants of follicular eczema, along with lichen spinulosus and juxtaclavicular beaded lines [7]. Its treatment also varies with different authors claiming response to steroids [1], isotretinoin, UVA therapy [8], keratolytics and tetracyclines [9]. We describe a case of localized infundibulofolliculitis of the neck diagnosed in a 21 year old female who was successfully treated with a course of topical tretinoin 0.025%. The presenting history, clinical findings, biopsy results and available literature are reviewed.
Case Report
A 21 year old girl presented to our out patient department with complaints of multiple tiny papules present around the neck since 2 years. The lesions were not associated with itching or pain. She denied application of any topical agents or prolonged exposure to sunlight. She did not give history of atopy. On examination, multiple, discrete hyperpigmented follicular keratotic papules and few discrete pustules were present around the neck extending from the nape of the neck, lateral and anterior aspects upto the supra sternal space (Fig. 1a,b). There were no other lesions anywhere on the body. Examination of the mucus membranes, hair and nails were normal.
Following differential diagnoses were considered:
1. Infundibulofolliculitis.
2. Pityrosporum folliculitis.
3. Kertosis Pilaris.
4. Pityriasis Rubra Pilaris.
5. Darier’s Disease. Screening for HIV and Syphilis was negative.
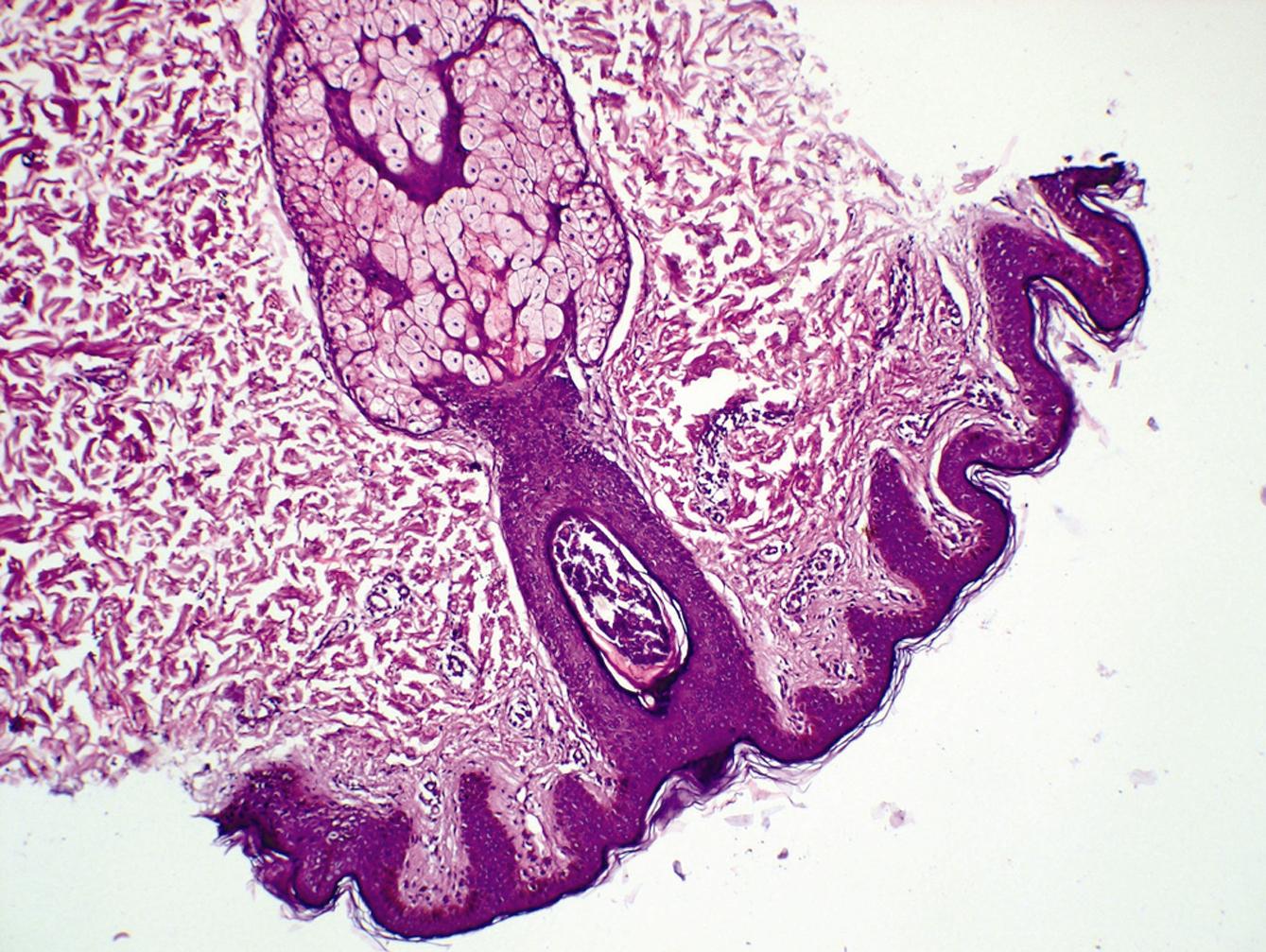
Scrapings obtained for KOH examination were negative. A punch biopsy of the lesion was obtained which showed multiple polymorphs around the infundibular part of the hair follicle (Fig. 2a,b) suggestive of diagnosis of infundibulofolliculitis. Clinical findings and histopathology report were suggestive of infundibulofolliculitis. The patient was treated with a two week course of topical tretinoin 0.025% followed by prompt resolution of the lesions (Fig. 3).
 |
 |
Figure 1a,b. Composite photograph showing multiple, discrete hyperpigmented follicular keratotic papules and
few discrete pustules localized to the neck
 |
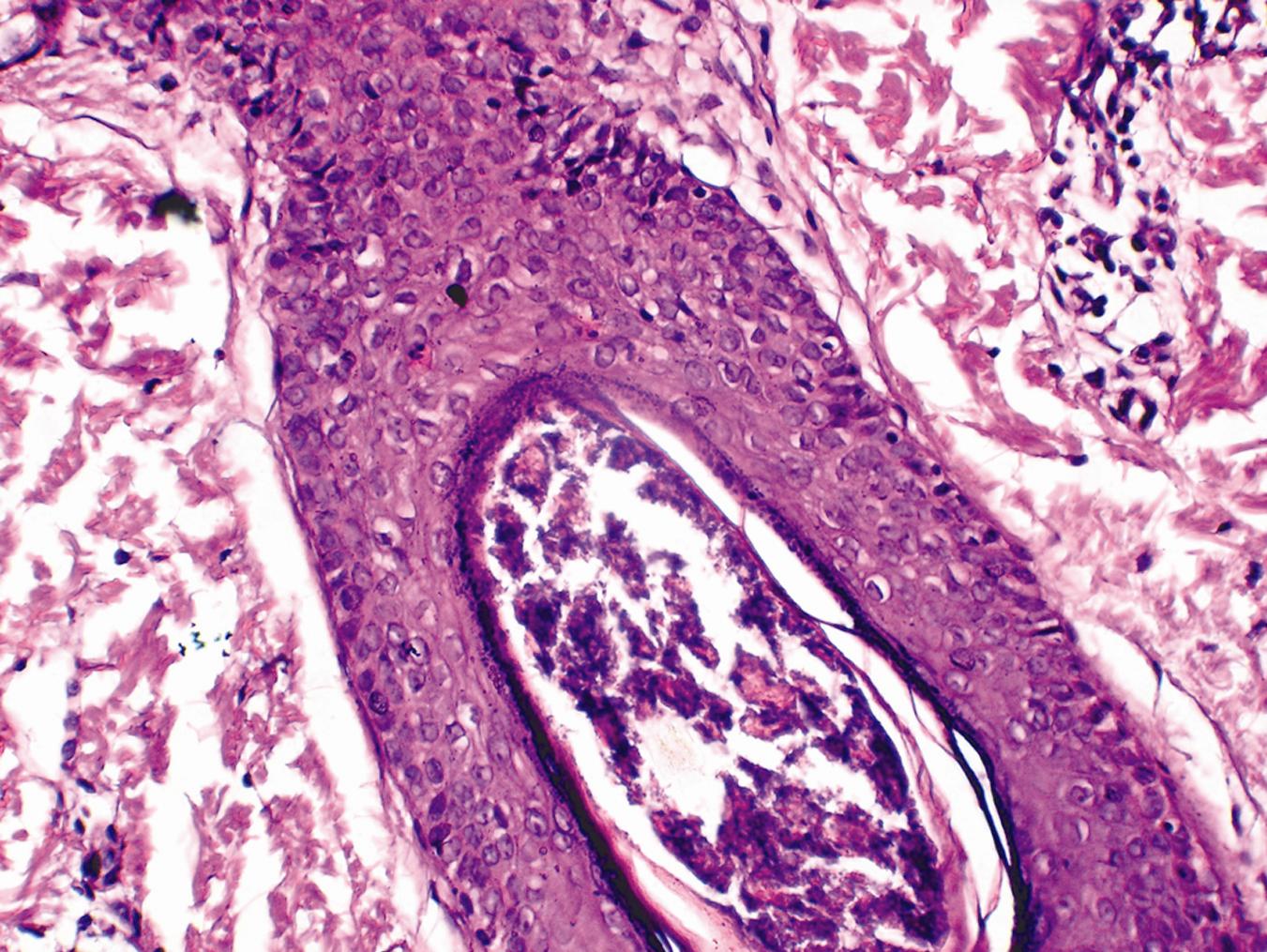 |
Figure 2a,b. Histopathology of biopsy H and E. (10x and 45x)
 2a,b. Histopathology of biopsy H
|
Discussions
DRIF is an uncommon pruritic follicular eruption of unknown etiology that is predominantly seen in black men [3]. This condition tends to affect the trunk and the upper extremities and is usually unresponsive to local and systemic treatment. In 1968, Hitch and Lund coined the word disseminated and recurrent infundibulofolliculitis for a patient who had presented with a diffuse, pruritic, skin colored, uniform follicular papular eruption with histologic findings of a perifollicular lymphocytic infiltrate and edema around the infundibular portion of the follicle [1]. Reports of patients with similar symptoms have been described as early as 1959 [1]. Because of the unique combination of clinical and histologic features, a consensus regarding its etiology has not been reached. An atopic etiology [5] has been suggested but refuted by many [6], as a family history is not available. An infectious etiology has also been considered [6] but given that the lesions disappear without antibiotics, it is unlikely. Also there is no evidence clinically or by biopsy of a fungal infection. DRIF has often been reported to be resistant to treatment. Failure with bland topical agents, antihistamines, tetracyclines, keratolytics and topical retinoin acid [9] has been reported. Mixed results have also been reported with oral vitamin A alone and in combination with vitamin E [3,6]. Topical steroids [9] and tretinoin creams have shown to be of variable effectiveness. Our patient presented with papular lesions around the neck which on biopsy was suggestive of infundibulofolliculitis. She was treated with a two-week course of 0.025% topical tretinoin and responded well (Fig. 3). She is currently asymptomatic. Recurrent or persistent disseminated infundibulofolliculitis remains a distinct entity best understood as a specific clinicopathologic response to an unknown cause or causes. Response to therapy is poor, although we report successful therapy with.
Conclusions
1. This case is being reported for its rarity in Caucasian females and only around the neck.
2. Successful therapy with topical tretinoin.
Acknowledgement
r. Sujatha C, Professor and Head of the Department of Dermatology, MVJ Medical College and Research Hospital.
Dr. Padmini Jeyachandran, Professor and Head of the Department of Pathology, MVJ Medical College and Research Hospital.
Dr. S Vasantha Kumar, Principal, MVJ Medical College and Research Hospital.
REFERENCES
1. Hitch JM, Lund HZ: Disseminate and recurrent infundibulofolliculitis: Report of a case. Arch Dermatol. 1968; 97: 432-435. 2. Heymann WR: Infundibulofolliculitis of the neck. Cutis. 2002; 70: 178-180. 3. Aroni K, Grapsa A, Agapitos E: Disseminate and recurrent infundibulofolliculitis: response to isotretinoin. J Drugs Dermatol. 2004; 3: 434-435. 4. Calka O, Metin A, Ozen S: A case of disseminated and recurrent infundibulofolliculitis responsive to treatment with systemic isotretinoin. J Dermatol. 2002; 29: 431-434. 5. Thew MA, Wood MG: Disseminate and recurrent infundibulofolliculitis: Report of a second case. Arch Dermatol. 1969; 100: 728-733. 6. Owen WR, Wood C: Disseminate and recurrent infundibulofolliculitis. Arch Dermatol. 1979; 115: 174-175. 7. Hay JB, Adriaans BM: Bacterial infections Blackwell Science Ltd, 998, pp: 1097-1179 . 8. Ravikumar BC, Balachandran C, Shenoi SD, Sabitha L, Ramnarayan K: Disseminate and recurrent infundibulofolliculitis: response to psoralen plus UVA therapy. Int J Dermatol. 1999; 38: 75-76. 9. Hinds GA, Heald PW: A case of disseminate and recurrent infundibulofolliculitis responsive to treatment with topical steroids. Dermatol Online J. 2008; 14: 11.
Comments are closed.