Our Dermatol Online. 2012; 3(1): 43-45
Date of submission: 22.10.2011 / acceptance: 25.11.2011
Conflicts of interest: None
POROID HIDRADENOMA: A CASE REPORT
POROID HIDRADENOMA: OPIS PRZYPADKU
Mona Mlika1, Beya Chelly1, Aida Ayadi-Kaddour1, Sadok Boudaya2, Tarek Kilani2, Faouzi El Mezni1
1Department of Pathology, Abderrahman-Mami Hospital – Ariana, University of Medicine El Manar, Tunis. Tunisia
2Department of Cardio-Thoracic Surgery, Abderrahman-Mami Hospital – Ariana, Tunis, Tunisia
Corresponding author: Dr. Mona Mlika e-mail: mlika.zorgati.mona@hotmail.com
How to cite an article: Mlika M, Chelly B, Boudaya S, Ayadi-Kaddour A, Kilani T, El Mezni F. Poroid hidradenoma: a case report. Our Dermatol Online 2012; 3(1): 43-45.
Abstract
Introduction: Poroid hidradenoma is a variant of the eccrine poroma that belongs to the group of poroid neoplasm. It presents architectural features of hidradenoma and cytologic features of poroid neoplasm. To date, very few cases of this entity have been reported in the literature. Case presentation: An eighty-one-year-old man whose past medical history was consistent for a Parkinson’s disease presented with a presternal nodular mass. Physical examination revealed a 6 cm, painless, and pedunculated presternal tumefaction. Chest Ultrasound examination revealed a heterogeneous tumor with anechoic areas and cystic component. CT-scan showed a presternal subcutaneous mass presenting a dual component sloid and cystic with stigmates of recent bleeding. A total surgical excision was performed and histologic examination concluded to a poroid hidredenoma. Conclusion: Poroid hidradenoma is the newest variant added to poroid neoplasm. Histologic characteristics may be challenging necessitating a thorough sampling. Treatment is based on surgical resection in order to to prevent from a possible recurrence or malignant transformation.
Key words: poroid hidradenoma; eccrine poroma; surgical resection
Introduction
Eccrine gland-derived lesions make up a large and relatively common group of adnexal tumors. Hidroacanthoma simplex, dermal duct tumor and eccrine poroma form a fairly homogeneous family derived from eccrine duct and pore. They belong to the poroid neoplasm group that represents 10% of sudoriferous tumors. Poroid hidradenoma is a recently recognized variant of poroid neoplasm that should be differentiated from apocrine hidradenoma [1]. It is a benign neoplasm with eccrine differentiation, originally described by Abenoza and Ackerman in 1990. Since then, less than 20 cases of poroid hidradenoma have been reported in the literature.
Case Report
An eighty-one-year-old man whose past medical history was consistent for a Parkinson’s disease, consulted for a pre-sternal lesion which appeared few years ago and has been growing gradually. Physical examination revealed a 6 cm and painless, pedunculated, presternal tumefaction with a hard consistency. Chest-X-ray was normal. Chest ultrasound examination revealed a heterogeneous tumor with anechoic areas and a cystic component. CT-scan showed a presternal subcutaneous mass presenting two components cystic and massive with stigmate of recent bleeding (Fig. 1a). Facing the radiologic findings, the diagnosis of a vascular tumor was initially suspected. A radical surgical excision was performed. On gross examination, we received a 6-centimeter mass with both solid and cystic components (Fig. 1b). Microscopic examination revealed a well demarcated and symmetrical tumor with eccrine differentiation situated in the dermis without connection to the overlying epidermis (Fig. 1c). This tumor presented architectural features of hidradenoma with tumor cells confined entirely within the dermis in both solid and cystic components and cytological features of a poroid neoplasm with poroid and cuticular cells showing ductal differentiation (Fig. 1d,e). At higher magnification, poroid cells had scanty cytoplasm and an oval to round nucleus with inconspicuous nucleoli. Cuticular cells had abundant and eosinophilic cytoplasm in which a larger nucleus was present (Fig. 1f). Neither atypical cells nor necrotic changes were observed. The patient was discharged few days later with no complications reported. The surgical wound healed in 2 weeks with normal scarring.
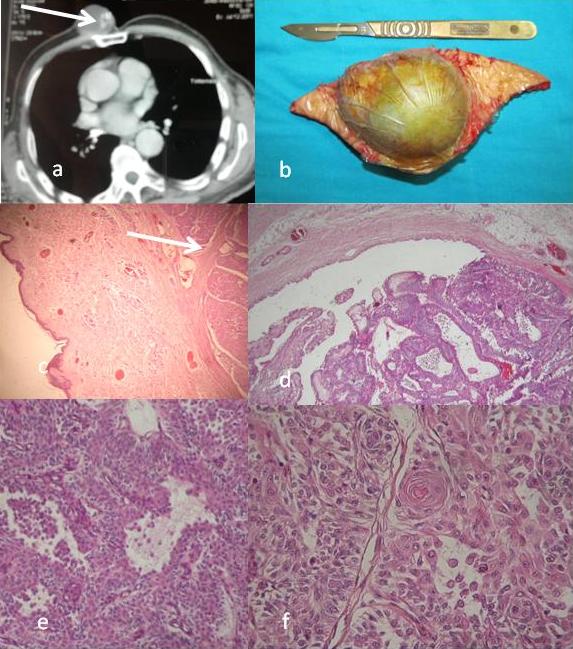 Figure 1. a: CT-scan showing a pre-sternal mass presenting two components cystic and massive. b: Gross features of a 6- centimeter sub-cutaneous mass with both solid and cystic components. c: Microscopic findings of a sub-cutaneous mass (HE x 250). d: Microscopic findings of a sub-cutaneous mass confined entirely within the dermis with both solid and cystic components (HE x 250). e: Microscopic findings showing a poroid neoplasm with poroid and cuticular cells showing ductal differentiation (HE x 400). f: Poroid cells had scanty cytoplasm and an oval to round nucleus with inconspicuous nucleoli. Cuticular cells had abundant and eosinophilic cytoplasm in which a larger nucleus is present (HE x 400)
|
Discussion
Poromas are benign neoplasms composed of poroid and cuticular cells. Four histopathologic variants are identified according to the architectural features of the neoplasm: hidradenoma simplex or intraepidermal poroma, eccrine poroma, dermal duct tumor and poroid hidradenoma [2]. Poroid hidradenoma is an uncommon variant of the eccrine poroma described by Abenoza and Ackerman in 1990. It is usually a solitary asymptomatic neoplasm that rarely becomes malignant in less than 1% of cases. The age of presentation varies from 28 to 77 years, with a peak of incidence in the seventh decade [3]. Its incidence is approximately equal in male and female patients. There is no predilection as to where the solitary lesion might occur. Typically poroid hidradenoma presents as a solitary, tender papule or nodule, well circumscribed and wholly intra-dermal, with a diameter ranging from 1 to 2 cm. It appears slightly reddish but the presence of cystic parts may confer a blue color on the lesion caused by the Tyndall phenomenon [1]. This was the case in our observation. In fact, the tumor contained two components: one solid and one cystic. Histologic examination showed that this neoplasm presents architectural features of hidradenoma, with solid and cystic areas and tumor cells restricted to the dermis (without connection to the epidermis), and cytological features of poroid neoplasm such as poroid and cuticular cells [4]. It is composed of cells similar to those in the uppermost segment of the intradermal eccrine duct and in the lower segment of the intraepidermal (acrosyringeal) eccrine duct. The poroid cells had scanty cytoplasm and an oval to round nucleus with inconspicuous nucleoli. Cuticular cells had voluminous and eosinophilic cytoplasm in which a larger nucleus with occasional multinucleation, resembling cuticles of eccrine duct [5]. Immunohistochemical study based on the keratin revealed that the neoplastic cells in eccrine poromas are considered to be closely related to the cells of dermal sweat ducts. Also the cuticular cells are considered to occupy an intermediate spectrum between the inner and outer cells of the dermal ducts [6]. The diagnosis of poroid hidradenoma is based on histologic examination of tissue samples; however, fine needle aspiration cytology (FNAC) can be useful in the diagnosis of cutaneous lesions especially in cases with cyst formation [5]. The differential diagnosis include other poromas such as hidroacanthoma simplex which is characterized by nests of round cells within the normal epidermal cells; dermal duct tumor which have histopathologic features of hidroacanthoma simplex but with the tumor cells located in the dermis; and eccrine poroma which is a lesion characterized by a clear margin between normal epidermal keratinocytes and a population of smaller cuboidal cells usually with darker nuclei protruding down into the underlying dermis. Apocrine hidradenomas are also considered as possible differential diagnoses. They account for 95% of all hidradenomas and have apocrine differentiation and. They are characterized by mucinous, polygonal and clear cells with areas of tubular differentiation. Some benign subcutaneous connective neoplasms such as fibroma, fibrolipoma, dermatofibroma, hemangioma, pyogenic granuloma, epidermal inclusion cyst, basal cell epithelioma and malignant eccrine poroma may also be challenging and may cause confusion with poroid hidradenoma [1]. The treatment of poroid hidradenoma is surgical including total excision of the lesion in order to prevent its recurrence. The prognosis of poroid hidradenoma is fairly good, and recurrence has been reported in only one case [5]. It is a benign tumor that can be easily misdiagnosed as a malignant neoplasm. This fact makes the thourough sampling and histologic examination mandatory in order to establish the diagnosis.
Conclusion
Poroid hidradenoma is the newest addition to the group of poromas. It is rarely reported in the literature. The diagnosis is made based on histologic findings. It is usually a benign neoplasm which needs surgical treatment consisting in total excision of the lesion in order to prevent recurrence and possible malignant transformation.
REFERENCES
1. Delfino S, Toto V, Brunetti B, Di Marino MP, Baldi A, Persichetti P: Poroid hidradenoma: A case report. In vivo 2007; 21: 905-908.
2. Rutten A, Requena L, Requena C: Clear-cell porocarcinoma in situ: a cytologic variant of porocarcinoma in situ. Am J Dermatopathol. 2002; 24: 59-62.
3. López V, Santonja N, Calduch-Rodríguez L, Jordá E: Poroid hidradenoma in a child: An unusual presentation. Pediatric Dermatology. 2011; 28: 1.
4. Requena L, Sanchez M: Poroid hidradenoma: a light microscopic and immunohistochemical study. Hautarzt. 1991; 42: 692-699.
5. Hoshida Y, Hanai J, Matsushita N, Yonekawa M, Kobayashi Y, Kawakami H, et al: Poroid hidradenoma: Report of a case with cytologic findings on fine needle aspiration. Acta Cytol 1999; 43: 471-474.
6. Yamamoto O, Hisaoka M, Yasuda H, Kasai T, Hashimoto H: Cytokeratin expression of apocrine and eccrine poromas with special reference to its expression in cuticular cells. J Cutan Pathol. 2000; 27: 367-373.
Comments are closed.