Our Dermatol Online. 2012; 3(1): 17-20
Date of submission: 18.07.2011 / acceptance: 25.10.2011
Conflicts of interest: None
TYPE 2 LEPRA REACTION (ENL) PRESENTING WITH EXTENSIVE CUTANEOUS ULCERATIONS
Hosahalli Rajaiah Yogeesh1, Sujatha Chankramath1, Hari Kishan Kumar Yadalla1, Shameem Shariff2, Suhas Bettadapura Ramesh1,
Sapnashree Budhnoor Sreekantaiah1
1Department of Dermatology, M.V.J. Medical College & Research Hospital, Hoskote, Bangalore, Karnataka, India
2Department of Pathology, M.V.J. Medical College & Research Hospital, Hoskote, Bangalore, Karnataka, India
Corresponding author: Dr. Hosahalli Rajaiah Yogeesh e-mail: hryogesh@yahoo.com
How to cite an article: Yogeesh HR, Chankramath S, Yadalla HKK, Shariff S, Ramesh SB, Sreekantaiah SB. Type 2 lepra reactions (ENL) presenting with extensive cutaneous ulcerations. Our Dermatol Online 2012; 3(1): 17-20.
Abstract
A 45 year old lady presented with multiple painful necrotic ulcerations over the trunk, arms, thighs and gluteal areas of two months duration. She also had erythematous papules and pustules over the face since 1 week. History of recurrent papular lesions, some of them undergoing ulceration were present since 3 years. All biochemical parameters were within normal limits. Rheumatoid factor, ANA, Elisa for HIV and VDRL were negative. Pus culture showed growth of Staphylococcus aureus. Smear for AFB showed multiple globi. Skin biopsy showed atrophic epidermis with grenz zone; dermis showed sheets of foamy macrophages and oedematous blood vessels infiltrated with neutrophils and ocasional plasma cells. Patient was admitted and was started on MDT-MB along with thalidomide and prednisolone.
Key words: type 2 Lepra reaction; necrotic ulcers; AFB; MDT
Introduction
Type 2 lepra reaction, otherwise termed erythema nodosum leprosum, is an acute inflammatory reaction seen in patients with lepromatous leprosy or occasionally in borderline lepromatous leprosy. Though it is usually seen during the course of treatment it may occur in previously untreated patients as well. The lesions described in type 2 reactions are erythematous painful tender papules and nodules. In mild reaction nodules are small in number and spontaneously resolve leaving behind hyperpigmented macules. In severe reactions, nodules tend to increase in size and ulcerate. Ulcerations heal with scarring. Sometimes erythema nodosum leprosum may be the presenting manifestation of leprosy [1]. Vesiculobullous, pustular, ulcerated, and hemorrhagic and erythema multiforme-like lesions have been reported in ENL (erythema nodosum leprosum) [2]. In this article, we have discussed a case which presented to us with severe skin ulcerations. The case was admitted in our hospital, MVJ medical college and research hospital, situated in the outskirts of Bangalore, where she was investigated and diagnosed and started on treatment. ;
Case Report
A 45 year old lady was brought to our OPD with multiple painful ulcerated skin lesions over the trunk, arms, thighs and gluteal area of 2 months duration. She also had multiple reddish eruptions and pustules over the face since 1 week; she gives history of recurrent attacks of papulo-pustular lesions, and ulceration since three years. Patient says that she was taking treatment from a doctor with partial subsidence of ulcers. It is possible that patient must have been put on steroid injections as history suggests. Six months ago she was diagnosed to have diabetes mellitus and she has been on irregular treatment for the same. In the present episode ulceration first started over the gluteal region and slowly developed over the other sites. According to the patient the present episode was the most severe one. Current episode is associated with history of fever since 1week – high grade and intermittent. No history of joint pains or abdominal symptoms suggestive of inflammatory bowel disease. On general physical examination, the patient was afebrile, vitals were stable,pallor was present and there were enlarged tender lymph nodes in the cervial, axillary and inguinal groups. Cutaneous examination revealed multiple erythematous indurated plaques surmounted with multiloculated ulcers of size varying from 1x1cm to 5x5cms, with undermined edges and covered with purulent discharge and crusts over both arms, forearms, thighs, abdomen and gluteal areas (Fig. 1,2). Forehead and both cheeks showed erythematous plaques with surmounted papules and pustules (Fig. 3). Multiple hypertrophic and keloidal scars were seen over both upper limbs and back (Fig. 4). Bilateral ulnar nerves, common peroneal nerves and supraorbital nerves were thickened and tender. Sensations could not be examined because of generalized cutaneous tenderness. Ophthalmic examination revealed no abnormality. Differential diagnosis of disseminated pyoderma gangrenosum and erythema nodosum leprosum and disseminated sweet’s syndrome was made and the patient was investigated.
 Figure 1. Clinical Photograph showing multiple plaques with ulcerations over abdomen, forearms and arm
|
 Figure 2. Clinical photograph showing ulcerations over the gluteal region
|
 Figure 3. Clinical photograph showing pustules and nodules on face
|
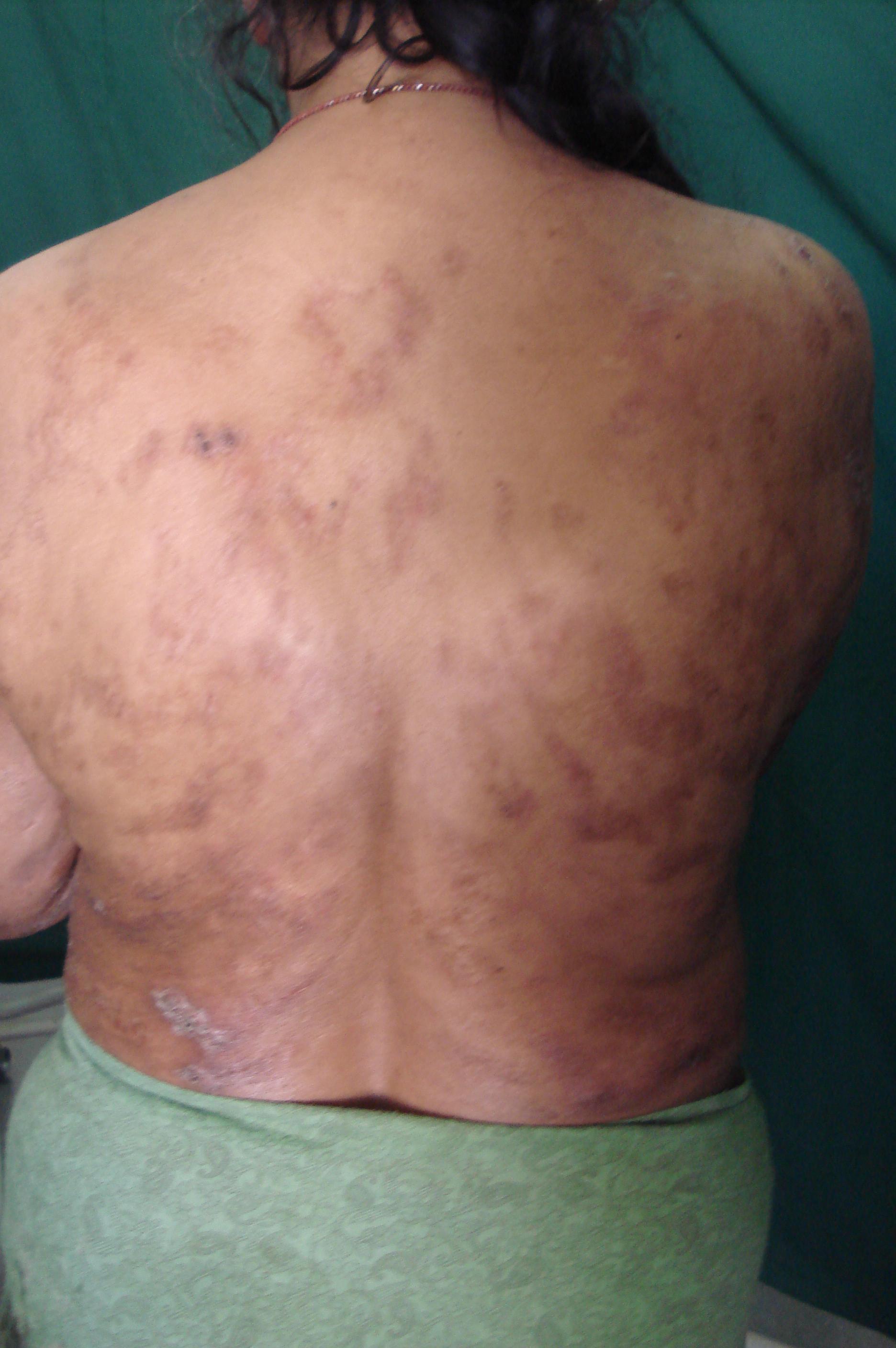 Figure 4. Clinical photograph showing scars an hyperpigmentation
|
Haematological investigations revealed Hb – 8.8gm%, TLC – 11000/mm3 with 78% of neutrophils, ESR showed 30mm in the 1st hour, FBS – 168mg% and PPBS – 295mg%. Urine analysis and all other biochemical parameters were within normal limits. Rheumatoid factor, ANA, HbsAg, Elisa for HIV and VDRL were negative. Pus culture showed growth of Staphylococcus aureus. Smear for AFB (acid-fast bacilli) showed multiple globi. Skin biopsy showed atrophic epidermis with grenz zone, dermis showed sheets of foamy macrophages intermingled with small aggregates of neutrophils and ocassional plasma cells, dermal vessels were oedematous and infiltrated with neutrophils (Fig. 5,6). Fite faraco stain showed macrophages packed with AFB (Fig. 7). A diagnosis of lepromatous leprosy with type 2 reaction was made and patient was started on MDT MB along with prednisolone 30mg and thalidomide 100mg tds. Patient did show some improvement; however she went against medical advice in spite of repeated requests and lost for follow up.
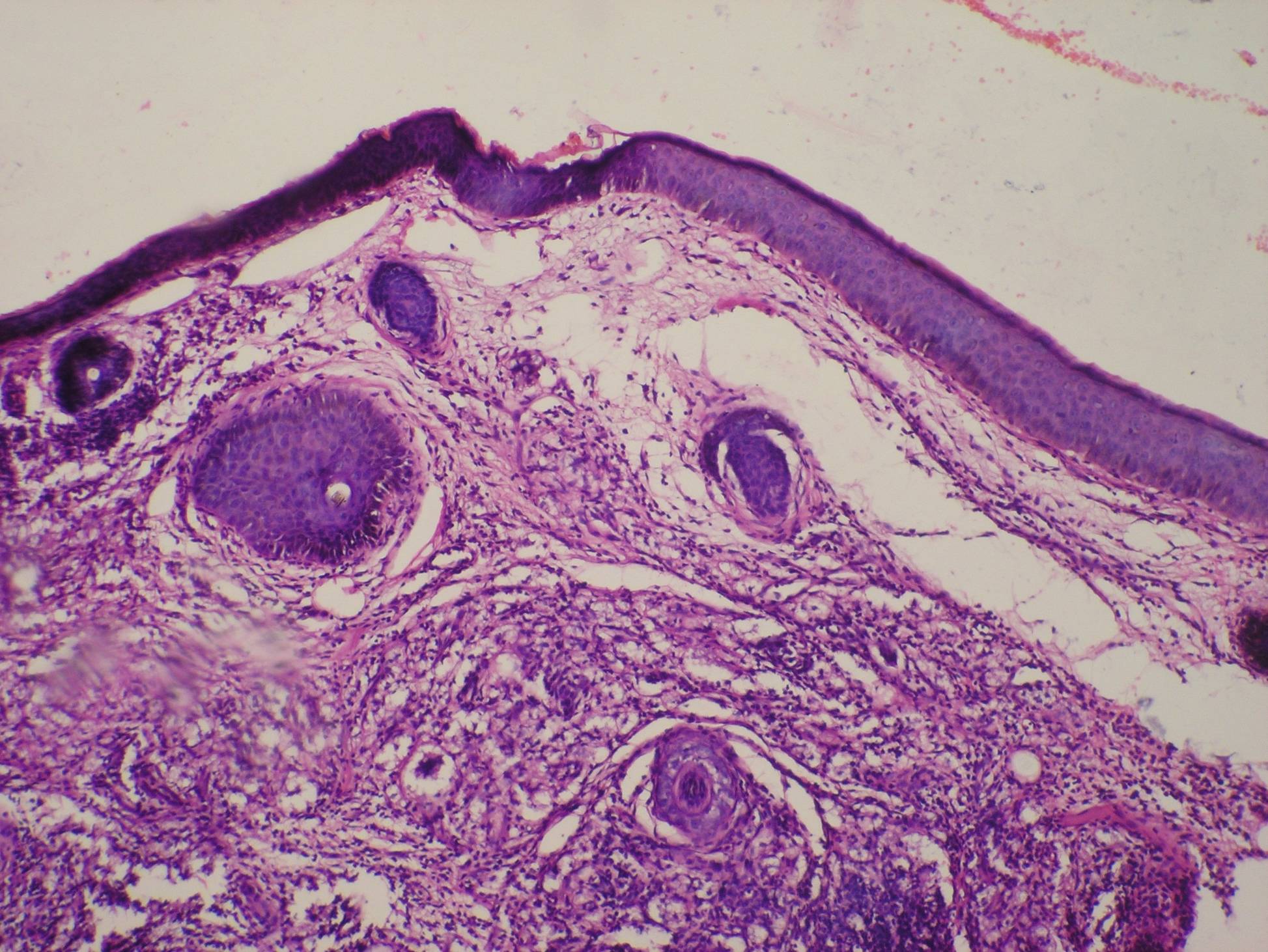 Figure 5. Histopathology (H&E) (100X)
|
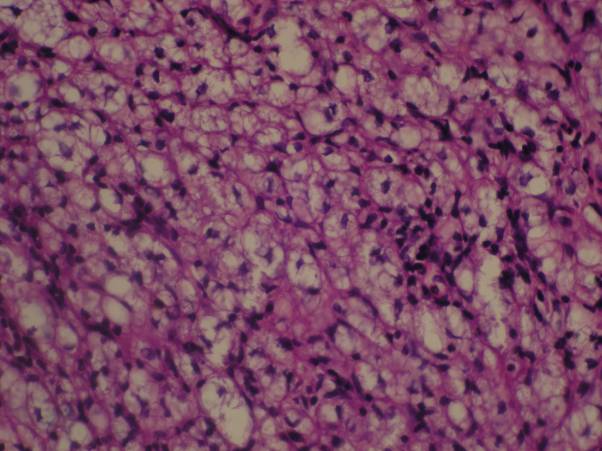 Figure 6. Histopathology showing sheets of foamy macrophages (H&E) (400X)
|
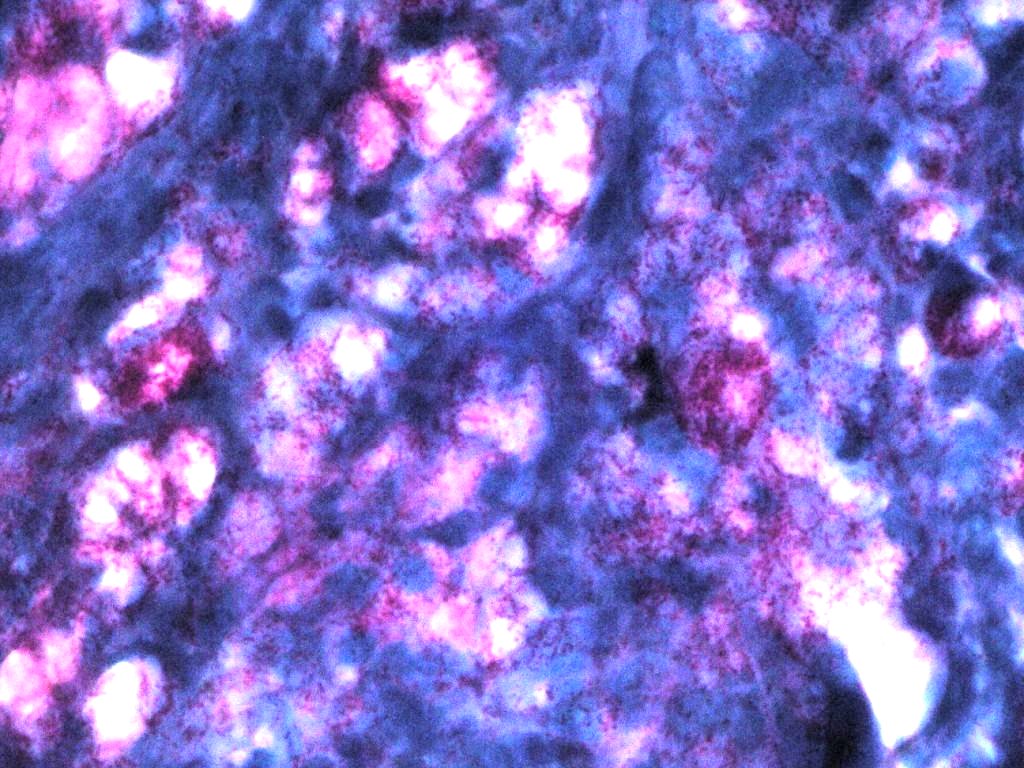 Figure 7. Fite-faraco stain of biopsy specimen showing AFB
|
Discussion
Leprosy is a chronic granulomatous infectious disease caused by Mycobacterium leprae. There is no other human infectious disease in which the clinical picture is as varied as leprosy. Type 2 lepra reaction is a type 3 Coomb and Gell hypersensitivity reaction usually seen in lepromatous and borderline lepromatous patients. It usually occurs later during the course of treatment and in longstanding untreated patients [2]. Antigen-antibody complexes are formed during the treatment in multibacillary leprosy and in patients with longstanding untreated disease with high bacillary load due to the death of bacilli; deposition of these complexes in various tissues causes inflammatory response with constitutional symptoms. Over half of Lepromatous leprosy and quarter of borderline lepromatous patients can develop type 2 reaction. In skin it presents most commonly with crops of multiple red dusky brown tender papules and nodules over the face and extensor aspects of the limbs. Lesions tend to recur at the same sites and if they do not resolve completely a chronic painful panniculitis develops which may persisit for months to years. Exacerbating factors for ENL are stress, pregnancy, lactation, concurrent illness and medication [3]. Arthritis, iritis, iridocyclitis and nephrits are other known features of ENL. ENL is more severe in caucasians and mongolians than in negroes. Ulceration occurs more readily and rapidly and unusual forms are seen. Various rare and atypical variants of ENL have been described in literature. Verma KK etal have reported necrotic erythema nodosum leprosum as a presenting manifestation of leprosy [4]. A rare variant of type 2 reaction characterised by pustular lesions on switching from WHO MDT to ofloxacin aided MDT was reported by Dave et al [5]. A persistent and localized variant of ENL was reported by S Prabhu et al [6]. Galvez et al reported an atypical evolution of BL as well as type 2 reaction primarily involving multiple nerves than skin [7]. A case of ENL clinically presenting as urticarial vasculitis that was then diagnosed to have LL has been reported by Funk WK et al [8]. Kou et al have reported a male with underlying lepromatous leprosy presenting with atypical reactional state simulating sweet syndrome [9]. A fatal case of erythema necroticans, the cause of death being septicemia secondary to skin ulcers and URTI ENL has been reported by Sethuraman et al and Petro et al [10,11]. This case is presented due to rarity of ENL leprosy presenting with such severe ulcerations, especially at a time when we have eliminated leprosy as a major health hazard in our country.
Conclusion
Although we encounter an occasional type 2 lepra reaction after initiating the multibacillary leprosy patients on MDT-MB, cases of ENL presenting with extensive cutaneous ulcerations are a very rare entity. However one should have a high index of suspicion in clinical practice failing which an easily treatable disease can be missed.
REFERENCES
1. Gomathy S, Divakaran J, Chakravarthy RS: Bullous erythema nodosum leprosum (bullous type 2 reaction). Int J of Dermatol 2002; 41: 363-364. 2. Meyerson MS: Erythema nodosum leprosum. Int J Dermatol 1996; 35: 389-392. 3. Pflatzgraff RE, Gopal R: Clinical leprosy. In: hastings RC, Opromolla DV A, ed. Leprosy. London: Churchill Livingstone, 1994: 237-287. 4. Verma KK, Pandhi RK: Necrotic erythema nodosum leprosum; A presenting manifestation of lepromatous leprosy. Int J Lepr Other Mycobact Dis 1993; 61: 293-294. 5. Dave S, Thappa DM, Nove AV, Jayanthi S: A rare variant of erythema nodosum leprosum: a case report. Dermatol Online J 2003; 9: 11. 6. Prabhu S, Rao R, Sripathi H, Rao L, Singh R: Localized and persistent erythema nodosum leprosum – a rare variant?. Dermatol Online J 2008; 14 :16. 7. Galvez J, Lopez-Dominguez JM, Navarro A, Creagh R, Casado JL, Chinchón Lara I: Patient with Hansen disease and lepromatous reaction with predominant neural involvement. Neurologia 1998; 13: 412-444. 8. Funk WK: Lepromatous leprosy and erythema nodosum. Hongkong dermatology and venereology bulletin 2001; 28- 30. 9. Kou TT, Chan HL: Severe reactional state in lepromatous leprosy simulating sweet`s syndrome. Int J Dermatol 1987; 26: 518-520. 11. Sethuraman G, Jeevan D, Srinivas CR, Ramu G: Bullous erythema nodosum leprosum (bullous type-2 reaction). Int J Dermatol 2002; 41: 363-364. 12. Petro TS: Bullous type of reaction mimicking pemphigus in lepromatous leprosy. Indian J Lepr 1996; 68: 179-181.
Comments are closed.