N Dermatol Online. 2011; 2(1): 3-7
Conflicts of interest: None
MUCORMYCOSIS IN HEMATOLOGIC PATIENTS: A REVIEW
García-Romero Maria Teresa1, García-Méndez Jorge2, Arenas Roberto3
1Departments of Dermatology, “Dr Manuel Gea González”, General Hospital. Mexico City
2Department of Infectious Diseases, Instituto Nacional de Cancerología Mexico City
3Departments of Dermatology and Mycology, “Dr Manuel Gea González”, General Hospital. Mexico City
Corresponding author: Dr. Arenas Roberto e-mail: rarenas98@hotmail.com
How to cite an article: García-Romero MT, García-Méndez J, Arenas R. Mucormycosis in hematologic patients: a review. Our Dermatol Online 2011; 2(1): 3-7.
Abstract
Most invasive fungal infections occur in patients with hematologic malignancies and the prevalence has increased steadily in recent years due to intensive cytotoxic chemotherapies, stem cell transplantation, myeloablative radiation therapy, and the use of corticosteroids, cyclosporine or new immunosuppressive agents. Although Candida is the main fungal agent involved in invasive fungal infection (IFI), an increasing number of infections are caused by molds, mostly Aspergillus spp, but in the last 20 years other emerging fungal pathogens such as Zygomycetes causing mucormycosis have appeared with higher mortality rates. The rhinocerebral and pulmonary forms of mucormycosis together with disseminated disease have the highest mortality (78-100%). Zygomycetes characteristically invade blood vessels, causing thrombosis and infarction with necrosis and scarring. Rapid diagnosis of zygomycosis is vital for management and therapy since these infections progress rapidly. Treatment should combine early aggressive surgical excision of the necrotic lesions, restoration of immune function if possible, and amphotericin B at a dose of 1-1.5 mg/kg or a new antifungal such as posaconazole.
Key words: zygomycosis; mucormycosis; lymphoproliferative disorders; immunosuppression
Introduction
Zygomycosis refers to a group of uncommon but aggressive infections caused by Zygomycetes, which is subdivided into two orders: the Entomophthorales and Mucorales. The angiotropic Mucorales, causing tissue necrosis, are frequently lethal in immunocompromised hosts and are grouped into the term mucormycosis [1,2]. Mucor spp, Rhizopus spp, Absidia spp and Rhizomucor spp are the most common causal agents [3]. Rhizopus oryzae, Rhizopus microsporus var. rhizopodiformis are the most commonly implicated (90%) [4], and occasionally have been implicated Absidia corymbifera (2-3%) [5], Cunninghamella spp, Apophysomyces spp and Saksenaea spp. These fungi are ubiquitous in the nature and are found in high-organic matter and soil [6,7], most of them are able to grow at more than 37’C [2]. They can be acquired by inhalation, ingestion, or infecting wounds [8], but their potential virulence in the human host is very low. They usually affect the immunocompromised patient including patients with hemato-oncologic diseases and transplant recipients, poorly controlled diabetics, iron overload states or treatment with deferoxamine [9] and extensive burns [2,10]. The use of broad-spectrum antibiotics has also been associated. Occasionally mucormycosis has been reported in immunocompetent patients following trauma. The main sites involved in cancer patients have been pulmonary, sinuses, sinopulmonary, rhinocerebral, disseminated, gastrointestinal tract, and soft tissues [11]; but rhinocerebral, pulmonary forms and disseminated disease have the highest mortality (78-100%) [8].
Discussion
Zygomycetes characteristically invade blood vessels, causing thrombosis and infarction with necrosis and scarring. This necrotic tissue favors fungal growth and limits penetration of systemic antifungals [5]. Rhinocerebral zygomycosis was classically described as occurring in patients with uncontrolled diabetes mellitus (with ketoacidosis). These patients typically present an advanced stage of the infection, and in most cases is usually fatal [12]. Nevertheless, more invasive fungal infections are being observed in immunocompromised patients over the past two decades. This trend is alarming because they are associated with significant morbidity and mortality. Two critical developments have contributed to this trend: an increase in the number of individuals with acquired immune deficits (cancer patients on systemic chemotherapy, solid and bone marrow transplant recipients and HIV disease) and aggressive therapeutic modalities like indwelling catheters, potent antineoplastic or immunosuppressive interventions and the widespread use of antimicrobial agents [13]. Along the last 50 years the classic manifestations and risk factors for zygomycosis in patients with cancer have been described: patients with leukemia using high-dose steroid or cytotoxic drugs, especially with purine analogs [14], and with prolonged neutropenia [7,15]. Zygomycetes are the second most frequent cause of opportunistic mold infections in hematologic malignancies; according to some series patients with acute leukemia are at highest risk [12,14]. The presentation most frequently encountered in these patients is the pulmonary form [11,14,16]. The infection rate is strongly correlated with the type of cytotoxic regimens administered and the duration of bone marrow aplasia [10]. One third of the patients have concomitant opportunistic fungal infections, reflecting svere immunosuppression [17]. The increased risk for developing zygomycosis involves two main processes: one is failure to clear and suppress fungal growth and failure to eliminate hyphae. Polymorphonuclear cells are the main host defense against filamentous fungi so functional or numerical deficiencies affecting them can result in invasive zygomycosis. Patients with hematological malignancies, such as leukemia, requiring potent cytotoxic regimens or with other causes of neutropenia (aplastic anemia) cannot generate an adequate response against fungi. Low serum pH diminishes the phagocytic and chemotactic ability of polymorphonuclears, hence the high prevalence in decompensated diabetic patients with hyperglycemia [2]. Also, the transferrin system is less functional at acid pH conditions, unbound iron circulates in the serum and is used by the fungus to grow which is the same phenomenon that occurs with deferoxamine therapy [2]. In one of the largest series of zygomycosis performed in a large tertiary cancer center, genotypic diversity of the causative Zygomycetes species by RTPCR showed lack of temporal-spatial clustering of the cases, making it unlikely that these infections were transmitted from a provider or other common source to the patients [18]. Recently it has been reported that the use of voriconazole prophylaxis for invasive aspergillosis in patients with hematologic neoplasias has increased the incidence of mucormycosis. A large series by Kontoyiannis et al found that voriconazole prophilaxis, diabetes mellitus and malnutrition were independent risk factors for zygomycosis in patients with leukemia or allogeneic bone marrow transplant (BMT) recipients [18,19]. The most common symptom of infection is fever (51%), especially while undergoing antimicrobial therapy [12,15]. Nevertheless, the symptoms vary according to the separate entities [10]. Sinusitis by zygomycetes should be suspected in patients with fever of unknown origin, sinus-nasal symptoms, mucosal discoloration or anesthetic necrotic regions of the face or oral cavity [20], any of these parts may contain necrotic areas that can be biopsied [21] (Fig. 1) allowing prompt clues to the diagnosis when trans-surgery studies are analyzed, including procedures such as KOH test. Zygomycetes enter the CNS through adjacent structures, such as paranasal sinuses or eye orbit where they can mimic a lymphoproliferative disorder (Fig. 2). Commonly such patients complain of facial or orbital pain. At physical examination there is some degree of proptosis, ophthalmoplegia, altered consciousness and nasal discharge [15]. Carotid artery thrombosis may occur. Patients with pulmonary infection usually are feverish and have mild to moderate hemoptysis. The most common imaging procedure (chest x-ray) rarely shows an air crescent sign, with is noteworthy [9,15]. Cutaneous mucormycosis can be primary or secondary to spread and can present as hemorrhagic and necrotic or nodular lesions or non-healing ulcers which can be misdiagnosed as hemorrhagic manifestations of the hematologic disease [8]. most common imaging procedure (chest x-ray) rarely shows an air crescent sign, with is noteworthy [9,15]. Cutaneous mucormycosis can be primary or secondary to spread and can present as hemorrhagic and necrotic or nodular lesions or non-healing ulcers which can be misdiagnosed as hemorrhagic manifestations of the hematologic disease [8]. In gastrointestinal tract involvement the main clinical signs are paralytic ileus and abdominal pain [22].
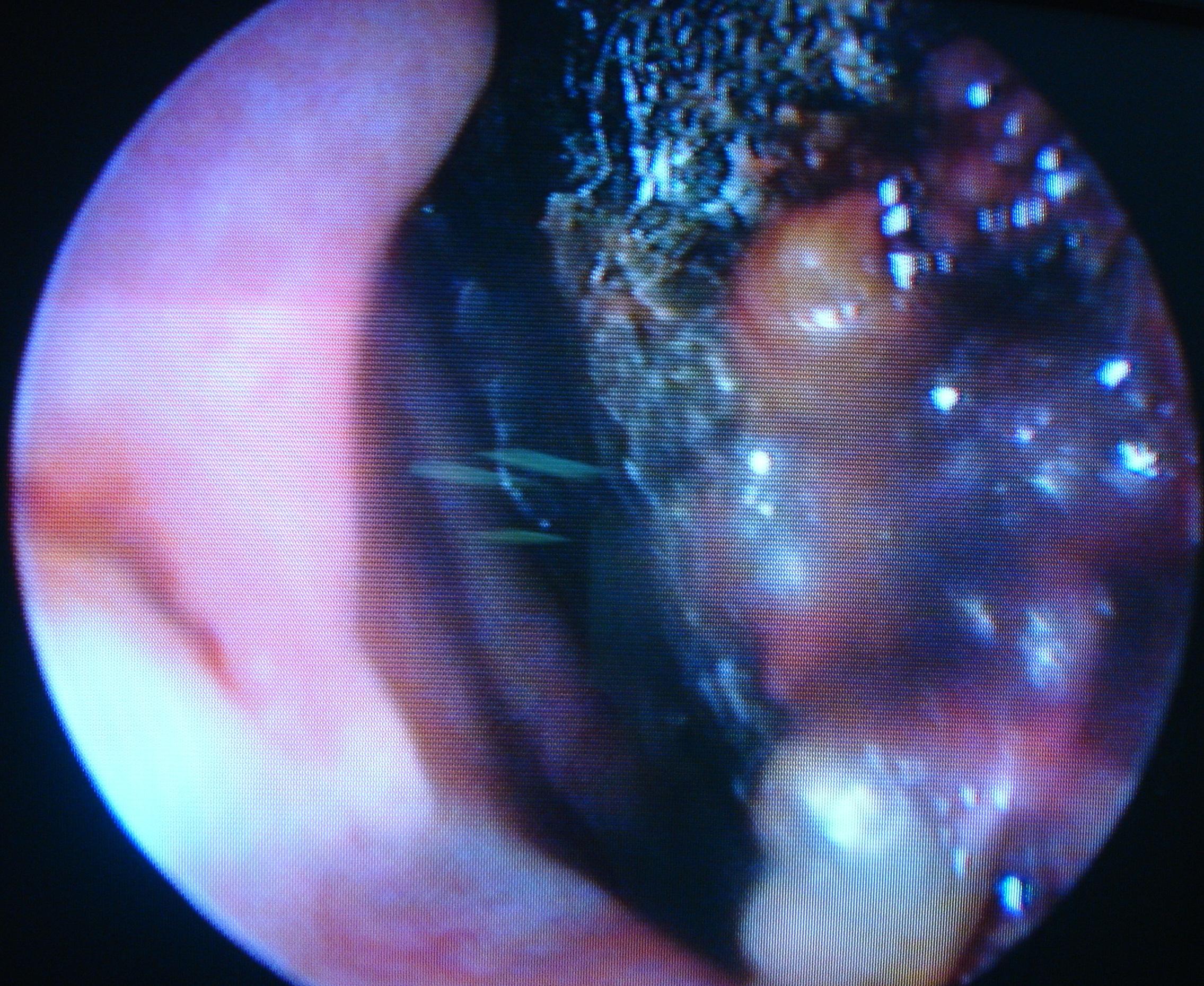 Figure 1. Necrotic sinus tissue found on endoscopy.
|
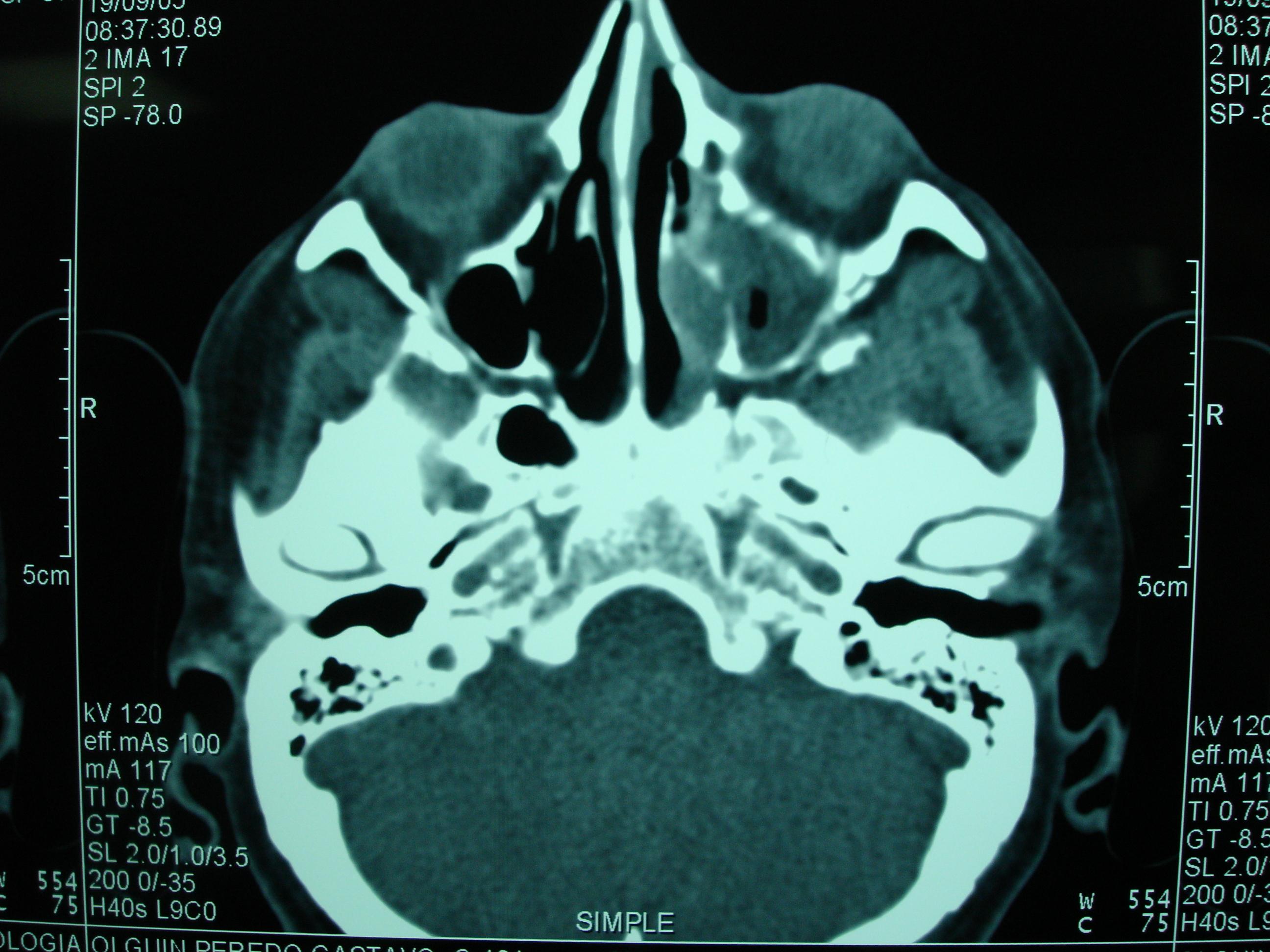 Figure 2. CT scan of a patient with invasion of left paranasal sinuses and orbit.
|
Rapid diagnosis of zygomycosis is mandatory for management and therapy since these infections progress rapidly [2]. Blood cultures are invariably negative (as in Aspergillosis), and sputum cultures and bronchial washings are seldom helpful [10]. Fungal elements are easily detected in biopsies, nasal scrapings or sputum. The key feature associated with the presence of Zygomycetes is the presence of wide, ribbon-like, non-septate, hyaline hyphae with KOH or Black Chlorazol [7] (Fig. 3). We must consider dermoscopy as an additional tool to improve diagnosis of zygomycetes in culture, because we can easily see the big sporangia through the glass of the culture tube [3] (Fig. 4). Most specimen samples sent to the pathology laboratory show large -10 to 20 μm in diameter- [10], pauciseptate rather than aseptate branching hyphae [23]. The inflammatory responses are predominantly neutrophilic [3], but can also be granulomatous, suppurative or absent (up to 20%). Invasive disease is characterized by prominent necrosis, vessel [3,12] and perineural invasion which should be carefully sought after [23]. Special stains like Gomori-Grocott and Schiff Peryodic Acid (PAS) should be used [3] (Fig. 5). Zygomycetes grow in 2 or 3 days (Fig. 6), and genera are identified by morphologic characteristics of their sporangia and sporangiophores. Rhizopus spp is characterized by cottony white colonies which later turn yellow or gray, darkly pigmented rhizoids and stolones, sporangiophores on the opposite, big round sporangia that break and leave the apophysis and collumelae shaped like a flat hat. Mucor spp produces cotton-like white colonies that darken with time, straight or ramified sporangiophores, big spherical sporangia with absence of apophysis that break and leave a collarete. They do not produce rhizoids or stolones and grow at 40’C (Fig. 7). Absidia spp also produces cotton-like white grayish colonies with small, pyriform sporangia, scant rhizoids and cone-like apophysis and collumelae. Rhizomucor spp is distinguished from Mucor by the presence of underdeveloped stolones and rhizoids and thermal tolerance of the 3 species [3](Fig.8).
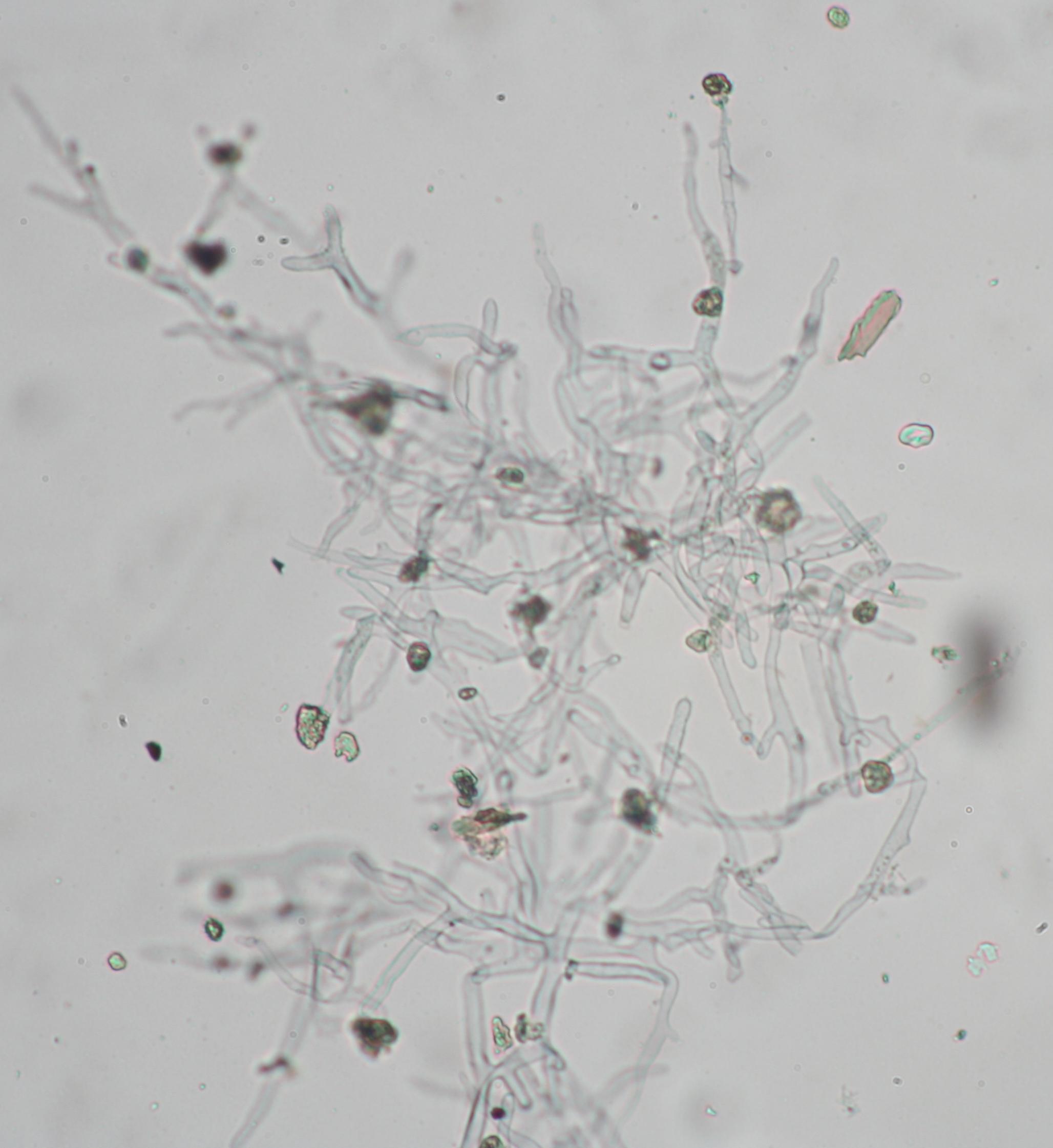 Figure 3. Mycologic exam with KOH showing wide, ribbon-like, nonseptate hyaline hyphae.
|
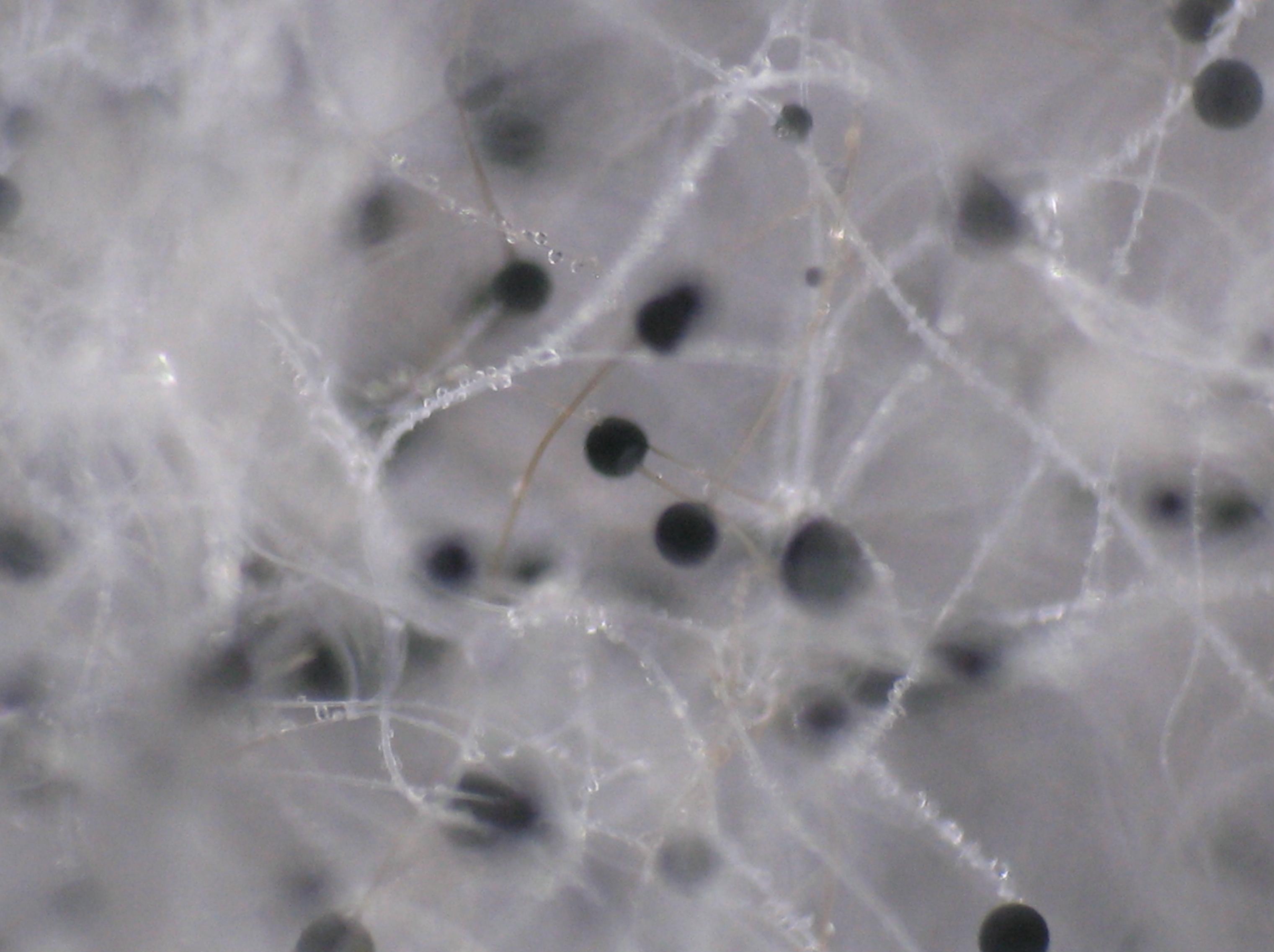 Figure 4. Dermoscopic view of big sporangia seen through the glass.
|
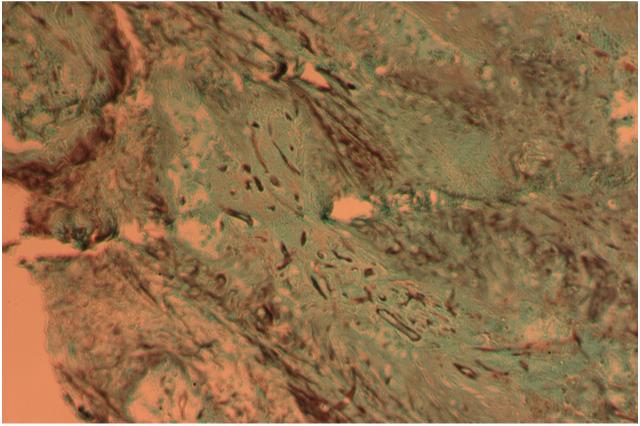 Figure 5. Biopsy with silver stain showing large pauciseptate hyphae invading tissue
|
 Figure 6. Zygomycete culture growing on bread.
|
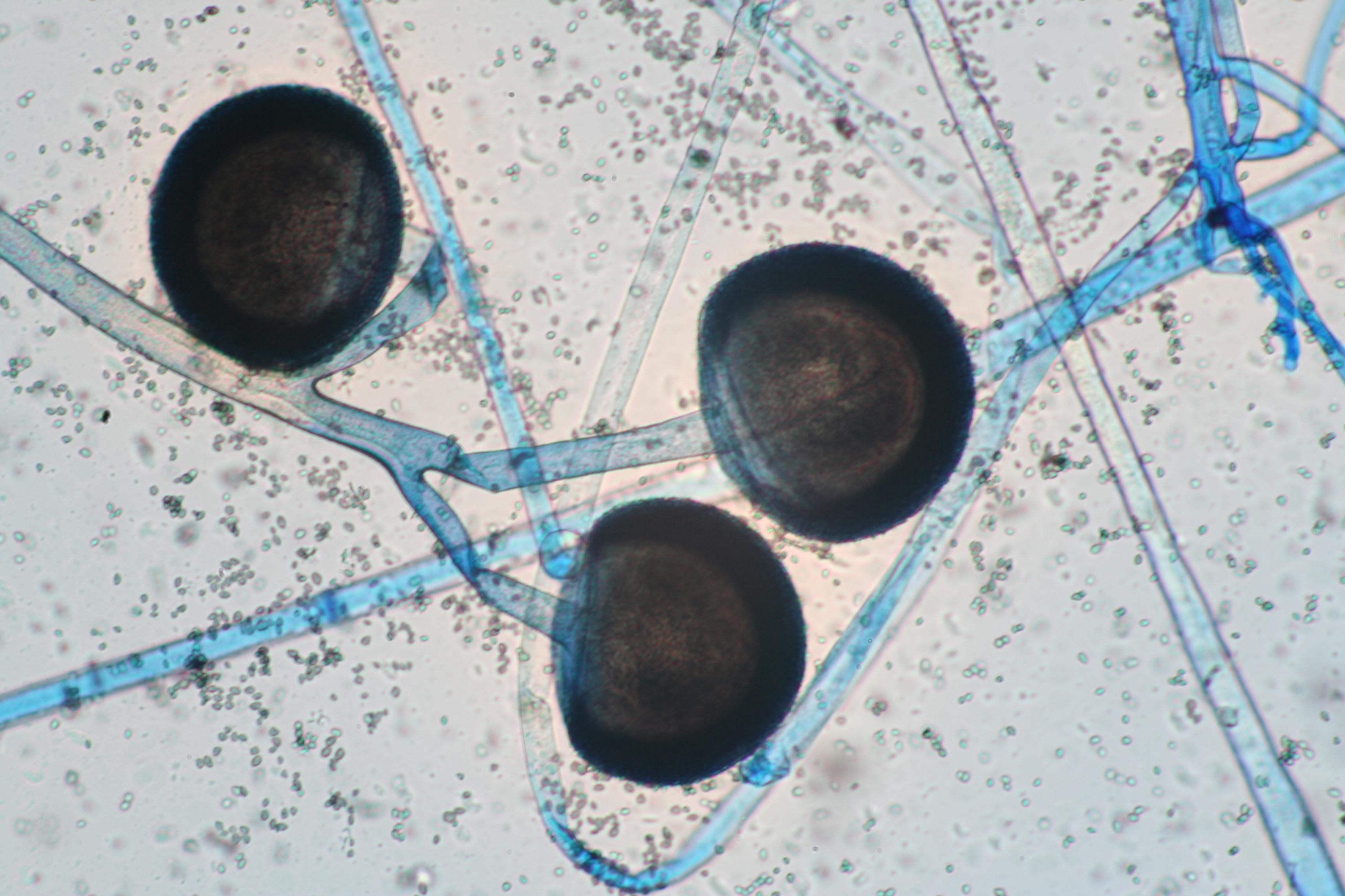 Figure 7. Sporangiophores with big sporangia, with no apophysis, rhizoids or stolones.
|
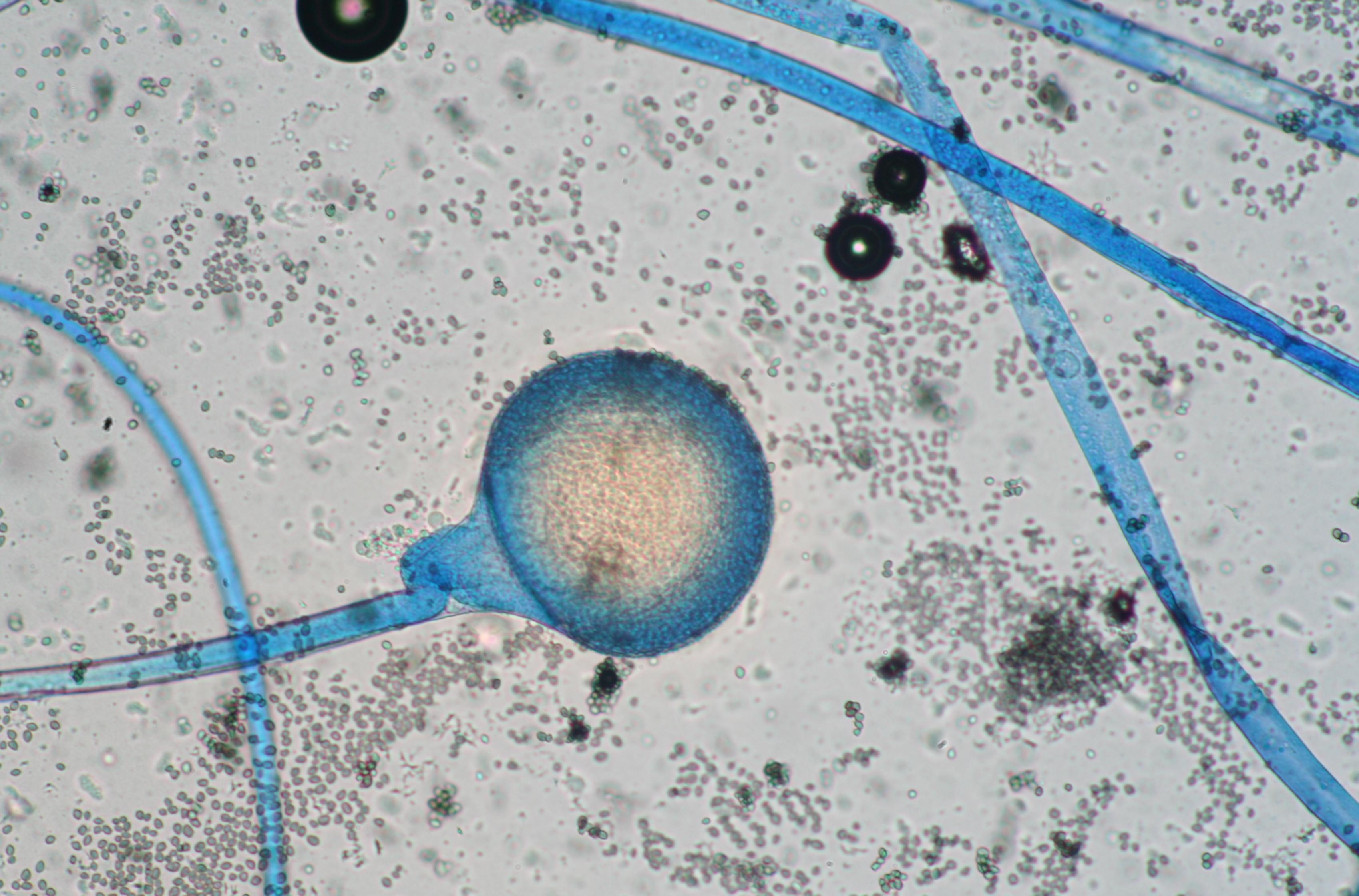 Figure 8. Sporangiophores with sporangia and underdeveloped stolones.
|
Only 30% of cultures are positive [3]. The asexual sporulating structures are rarely seen, but have been reported [6]. Currently new molecular techniques have been performed, for identification and differentiation between the different species, enabling early diagnosis such as direct PCR-RFLP [7] and internal transcribed spacer (ITS) [24]. Treatment should combine early aggressive surgical excision of the necrotic lesions, restoration of immune function if possible, high doses of amphotericin B (1-1.5 mg/kg) must be administered [2,12,15,16,22,25]. The duration of therapy is not clearly defined but prolonged treatment until remission is recommended [2]. There are reports of successful treatment with lipid formulations of amphotericin B (1-4 mg/kg) [12,16,26], WBC transfusions, hyperbaric oxygen [17] and colony-stimulating factors, have been proposed; but large series have shown no advantage of these modalities [11]. Specifically to reverse neutropenia, G-CSF, which promotes neutrophils proliferation and differentiation, has been successfully used in combination with amphotericin B [2,27]. Once the infection has been controlled, a chronic suppressive course with amphotericin B should be considered for as long as the immunosuppresion persists [2]. Among the new antifungal drugs, posaconazole has in-vivo action against Rhizopus species but other new azoles agents such as ravuconazole and voriconazole are inactive against Zygomycetes. None of the echinocandins tested are active against the Mucorales [18,28]. High rates of resistance against itraconazole have been reported [18], discouraging its use as a prophylactic agent. Indiscriminate prophylaxis with antifungals without activity against non-Aspergillus molds might result in selection of resistant molds, so risk-based approaches or drugs with activity against Zygomycetes such as posaconazole as a prophylactic agent should be considered in high-risk patients of invasive fungal infections [18,27].
Conclusion
The mortality rate among cancer patients with zygomycosis is high [22], in contrast to the relatively good prognosis in patients without an underlying malignant disease, even patients with diabetes mellitus [9,15]. Even with the appearance of new antifungal agents, recently one of the largest series reported a mortality rate of 64% among patients with hematologic malignancies diagnosed with zygomycosis [27]. The poor prognosis is explained mainly by delayed diagnosis and resistance of the fungi. This could be avoided with an emphasis in suspecting the zygomycete involvement promptly, looking for the usual sites (sinuses, pulmonary, gastrointestinal and rhinocerebral), and starting an appropriate antifungal agent (posaconazole or amphotericin B). Hyperacute disease and involvement of the lungs or ł 2 noncontiguous sites confers a poor prognosis [11].
REFERENCES
1. Kontoyiannis DP, Lewis RE: Invasive zygomycosis: Update on pathogenesis, clinical manifestations and management. Infect Dis Clin N Am 2006; 20: 581-607. 2. González CE, Rinaldi MG, Sugar AM: Zygomycosis. Infect Dis Clin N Am 2002; 16: 895-914. 3. Arenas R: Micología médica ilustrada: Zigomicosis. Mexico McGraw Hill 2008, 3rd ed: 247-264. 4. Bottone EJ, Weitzman I, Hanna BA: Rhizopus rhizopodiformis: emerging etiological agent of mucormycosis. J Clin Microbiol 1979; 9: 530-537. 5. Cloughley R, Kelehan J, Corbett-Feeney G, Murray M, Callaghan J, Regan P et al: Soft tissue infection with Absidia corymbifera in a patient with idiopathic aplastic anemia. J Clin Microbiol 2002; 40: 725-727. 6. Ciesla MC, Kammeyer PL, Yeldandi V, Petruzzelli GJ, Yong SL: Identification of the asexual state of Rhizopus Species on histologic tissue sections in a patient with rhinocerebral mucormycosis. Arch Pathol lab med 2000; 124: 883-887. 7. Machouart M, Larché J, Burton K, Collomb J, Maurer P, Cintrat A, et al: Genetic identification of the main opportunistic Mucorales by PCR-restriction fragment length polymorphism. J Clin Microbiol 2006; 44: 805-810. 8. Ameen M, Arenas R, Martínez-Luna E.: The emergence of mucormycosis as an important opportunistic fungal infection: five cases presenting to a tertiary referral center for mycology. Int J Dermatol 2006; 45: 1-5. 9. Lee FYW, Mossad SB, Adal KA.: Pulmonary mucormycosis: the last 30 years. Arch Intern Med 1999; 159: 1301-1309. 10. Sammassimo S, Mazzotta S, Tozzi M, Gentili S, Lenoci M, Santopietro R, et al: Disseminated Mucormycosis in a patient with acute myeloblastic leukemia misdiagnosed as infection by Enterococcus faecium. J Cin Microbiol 2004; 42: 487-489. 11. Kontoyiannis DP, Wessel VC, Bodey GP, Rolston KV: Zygomycosis in the 1990s in a tertiary-care cancer center. Clin Infect Dis 2000; 30: 851-856. 12. Lerchenmüller C, Göner M, Büchner T, Berdel WE: Rhinocerebral zygomycosis in a patient with actue lymphoblastic leukemia. Annals of Oncology 2001; 12: 415-419. 13. Roilides E, Lyman CA, Panagopoulou P, Chanock S: Immunomodulation of invasive fungal infections. Infect Dis Clin N Am 2003; 17: 193-219. 14. Pagano L, Caira M, Candoni A, Offidani M, Fianch L, Posteraro B, et al: The epidemiology of fungal infections in patients with hematologic malignancies: the SEIFEM-2004 study. Hematologica 2006; 91: 1068-1075. 15. Funada H, Matsuda T.: Pulmonary mucormycosis in a hematology ward. Internal Medicine 1996; 35: 540-544. 16. Nosari A, Oreste P, Montillo M, Carrafiello G, Draisci M, Muti G, et al: Mucormycosis in hematologic malignancies: an emerging fungal infection. Hematologica 2000; 85: 1068-1071. 17. Kontoyiannis DP, Lewis RE: Invasive zygomycosis: Update on pathogenesis, clinical manifestations and management. Infect Dis Clin N Am 2006; 20: 581-607. 18. Kontoyiannis DP, Lionakis MS, Lewis RE, Chamilos G, Healy M, Perego C, et al: Zygomycosis in a tertiary-care cancer center in the era of Aspergillus-active antifungal therapy: A case-control observational study of 27 recent cases. JID 2005; 191: 1350-1360. 19. Baddley JW, Stroud TP, Salzman D, Pappas PG: Invasive mold infections in allogeneic bone marrow transplant recipients. Clin Infect Dis 2001; 32: 1319-1324. 20. Epstein VA, Kern RB: Invasive fungal sinusitis and complications of rhinosinusitis. Otolaryngol Clin N Am 2008; 41: 497-524. 21. Pruitt AA: Nervous system infections in patients with cancer. Neurol Clin N Am 2003; 21: 193-219. 22. Bethge WA, Schmalzing M, Stuhler G, Schumacher U, Kröber SM, Horger M, et al: Mucormycoses in patients with hematologic malignancies: an emerging fungal infection. Hematologica 2005; 90: e62-e64. 23. Frater JL, Hall GS, Procop GW: Histologic Features of Zygomycosis: Emphasis on perineural invasion and fungal morphology. Arch Pathol Lab Med 2001; 125: 375-378. 24. Schwarz P, Bretagne S, Gantier JC, Garcia-Hermoso D, Lortholary O, Dromer F, et al: Molecular identification of zygomycetes from culture and experimentally infected tissues. J Clin Microbiol 2006; 44: 340-349. 25. Denning DW, Kibbler CC, Barnes RA: British Society for Medical Mycology proposed standards of care for patients with invasive fungal infections. Lancet Infect Dis 2003; 3: 230-40. 26. Pagano L, Offidani M, Fianchi L, Nosari A, Candoni A, Piccardi M, et al: Mucormycosis in hematologic patients. Haematologica 2004; 89: 207-214. 27. Martino R, López R, Sureda A, Nomdedeu J, Briones J, Martin-Henao G, et al: Risk of reactivation of a recent invasive fungal infection in patients with hematological malignancies undergoing further intensive chemoradiotherapy. Haematologica 1997; 82: 297-304. 28. Masiá-Canuto M, Gutiérrez-Rodero F: Antifungal drug resistance to azoles and polyenes. Lancet Infect Dis 2002; 2: 550-563.
Comments are closed.